Vaccine options
The development of effective vaccines to prevent paralytic polio was one of the greatest medical advances of the 20th century.
Today there are two types of vaccines against this disease. Inactivated polio vaccine (IPV), which contains killed poliovirus, is administered intramuscularly. Oral polio vaccine (OPV), which contains a weakened live poliovirus, is given by mouth. It is the most commonly used polio vaccine today. Vaccines can be divided into types. As a result of the development and evaluation of the bivalent oral polio vaccine in 2009, the Global Polio Eradication Initiative now has an arsenal of 5 different vaccines to stop polio transmission:
- oral polio vaccine (OPV);
- monovalent oral polio vaccine (mOPV1 and mOPV3);
- bivalent oral polio vaccine (bOPV);
- inactivated polio vaccine (IPV).
In Russia, until April 2021, the following mono- and combined vaccines were used to prevent polio: mono vaccines - oral polio types 1, 2, 3, Imovax Polio, Poliorix; combination vaccines - Infanrix Penta, Infanrix Hexa, Pentaxim, Tetraxim.
In April 2021, OPV containing Sabin strains 1, 2 and 3 was destroyed in accordance with the WHO Global Polio Eradication Initiative.
Principles and purposes of vaccination
Polio is a serious disease that affects the nervous system and can lead to paralysis in a matter of hours. Poliomyelitis is incurable, it can only be prevented. When given repeatedly, the polio vaccine can protect a child for life.
Vaccination against polio is carried out everywhere. According to the National Vaccination Calendar of the Russian Federation, the first two vaccinations are carried out with IPV, the third and subsequent revaccinations are carried out with OPV. In addition to vaccination and revaccination of children, revaccination of adults is carried out if they travel to areas dangerous for polio.
Currently, under the auspices of WHO, a program to eradicate polio from the Earth is being implemented. Russia is certified as a country free from wild poliovirus. But as long as there is at least one infected child in the world, children in all countries are at risk of contracting polio.
Failure to eradicate polio from these remaining persistent foci could result in up to 200,000 new cases of the disease occurring annually worldwide within 10 years.
Vaccine effectiveness
The introduction of vaccines that prevent polio into practice led to a rapid decrease in incidence, and in many territories to its almost complete elimination (for example, in the USSR since 1961). (Incidence fell from 22,000 cases to 4,000 cases in 1961; since 1962, no more than 100-150 cases have been reported per year, many of which may have been caused by other enteroviruses).
Since 1988, the number of polio cases worldwide has decreased by more than 99%, from an estimated 350,000 to 73 cases reported in 2015. This decrease was the result of global efforts to eradicate the disease. The polio vaccine forms long-term immunity to the virus of all types in 95% of those vaccinated after the first course of vaccination (three vaccinations).
Some countries have switched to inactivated polio vaccine only due to progress towards polio eradication (as the risk of wild poliovirus has decreased). But most countries use OPV because it has the unique ability to induce local gut immunity, meaning it can interrupt transmission of wild poliovirus in the natural environment. This is not possible with IPV, an inactivated polio vaccine that stimulates low levels of immunity against poliovirus in the intestine, resulting in individual protection against polio, but unlike OPV, it cannot prevent the spread of wild poliovirus. IPV is recommended for patients with immunodeficiency, HIV-infected people, as well as those whose families have such patients.
Causes
The causative agent of polio is three types of poliovirus. The source of infection is patients and virus carriers.
The virus is transmitted by the fecal-oral and airborne routes.
In tropical countries, cases of the disease are recorded throughout the year, in countries with temperate climates more often in summer and autumn.
Factors contributing to the spread of the virus:
- failure to comply with personal hygiene rules (dirty hands);
- poor removal of excrement;
- poor sewerage;
- contaminated food (unwashed vegetables and fruits) and water (including swimming in contaminated bodies of water);
- house flies.
Post-vaccination reactions
There is practically no reaction to the introduction of a live vaccine. In extremely rare cases, a slight increase in body temperature is possible 5-14 days after vaccination. In young children, a slight increase in bowel movements may occur, which lasts 1-2 days and goes away on its own without treatment. After administration of an inactivated vaccine, in a small percentage of cases there may be local reactions in the form of swelling and redness. Very rarely, a general reaction may occur in the form of a slight rise in body temperature, anxiety of the child on the first or second day after vaccination, which soon disappear.
Signs of infection after contact with a child who has been vaccinated
As mentioned earlier, if an infection occurs, then most likely the baby will experience it asymptomatically, or the negative manifestations will resemble a cold or intestinal infection.
But even if the worst thing happened, and the child fell ill with vaccine-associated paralysis (VAPP), this is not a death sentence.
The treated pathology (according to statistical data) leaves paralysis in only 25% of those who have recovered from the disease, and in more than 30% of cases it is cured without consequences.
How does polio manifest? Symptoms of this disease can be diagnosed at different time periods and directly depend on the route of infection. Typically, a vaccine recipient may develop signs of polio within 4-30 days after immunization.
However, if a child is infected through contact with a person vaccinated with a live vaccine, symptoms usually appear after two or three months. Interestingly, immunocompromised individuals may develop vaccine-associated polio after as long as six months.
Based on severity, doctors distinguish three main forms of VAPP:
- mild, passing after a month (abortive form);
- paralytic, causing the syndromes of the same name and increasing the fragility of bone tissue;
- and severe, capable of causing disability (muscle atrophy) or even death.
Symptoms of VAPP include:
- headache;
- increase in body temperature;
- muscle twitching;
- cough;
- pain in the back and limbs;
- rhinitis;
- insomnia (or vice versa, drowsiness);
- and dyspeptic disorders.
It should be noted that symptoms rarely last more than a month. But paralytic forms of VAPP are much more difficult for children to tolerate. Here the muscles of almost the entire body suffer greatly.
Vaccinated children are not dangerous to others. The exception is OPV vaccination. After this procedure, the patient releases viral strains into the environment for another 60 days. During this period, if there is close contact, an unvaccinated baby may become infected.
But if by this time he has already undergone 2-fold IPV vaccination, he will never get VAPP, which means he can safely contact people vaccinated with OPV. It should be remembered that a child can only get vaccine-associated polio if he has an immunodeficiency.
However, if there is even potential contact with a vaccinated OPV, the unvaccinated baby should be vaccinated.
If you refuse the procedure, be sure to separate the children for 2 months from the date of oral immunization.
Contraindications
For OPV:
- Neurological disorders accompanying previous vaccination with polio vaccine.
- Immunodeficiency state (primary), malignant neoplasms, immunosuppression (vaccinations are carried out no earlier than 6 months after the end of the course of therapy).
- Routine vaccination is postponed until the end of acute manifestations of the disease and exacerbation of chronic diseases. In case of mild ARI, acute intestinal diseases and other non-severe conditions, vaccinations are carried out immediately after the temperature has returned to normal.
The use of OPV is only possible in healthy children. Before vaccination, a doctor's examination is required.
For IPV:
- Diseases accompanied by an increase in body temperature, acute manifestations of an infectious disease or exacerbation of a chronic disease. In these cases, vaccination should be postponed until recovery;
- Allergic reaction to previous administration of the vaccine (allergy to the active component, to one of the excipients included in the vaccine - streptomycin, neomycin and polymyxin B);
Treatment of polio
Treatment of polio is carried out by an infectious disease specialist in a hospital setting.
Patients are isolated in a box for 40 days.
There is no specific treatment against the disease -
- symptomatic therapy is carried out (antipyretics, painkillers, sedatives),
- gammaglobulin and vitamin therapy (vitamins C, B1, B 12, B6), amino acids are prescribed.
Patients in the acute stage of the disease are prescribed strict bed rest (2-3 weeks). In case of paralysis of the respiratory muscles - artificial ventilation.
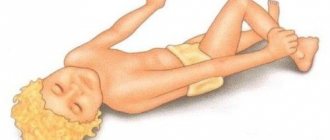
Paralyzed limbs require special attention. The positions of the legs, arms and spine must be correct. The legs are laid parallel, slightly bent at the knee and hip joints using pads. The feet should be perpendicular to the shins (they are fixed by placing a thick pillow under the soles). The arms are spread to the sides and bent at the elbow joints at an angle of 90°.
To improve neuromuscular conduction, prozerin, neuromidin, and dibazol are prescribed. Treatment in the infectious diseases department takes 3-4 weeks.
Rehabilitation treatment begins in the hospital and continues on an outpatient basis. Physical therapy is prescribed, classes are held with an orthopedist, water procedures (exercises under water), physiotherapy (UHF, electrical stimulation, applying hot wet compresses to sore muscles). In the future, sanatorium-resort treatment (sea, sulfur baths, mud) is indicated.
When to vaccinate?
According to the National Vaccination Calendar, the first IPV vaccination is carried out starting from 3 months, the second – at 4.5 months, the 3rd vaccination of the primary vaccination course is given at 6 months with live polio vaccine. Revaccinations against polio are carried out in accordance with the OPV calendar: the first - at 18 months, the second - at 20 months, the third - at 14 years.
When using inactivated polio vaccine in accordance with the instructions for the drug, the first revaccination is carried out 1 year after the third administration of the vaccine. Subsequent revaccination is carried out every 5 years until the patient reaches the age of 18 years and then every 10 years for life.
Diagnostics
When making a diagnosis, clinical, epidemiological, serological and virological data should be taken into account:
- spinal puncture (increased pressure of cerebrospinal fluid, leukocytes - neutrophils, increased protein content);
- general blood test (signs of inflammation: leukocytosis, increased ESR);
- throat washes and culture on a nutrient medium;
- fecal analysis with culture;
- culture of blood and CSF on a nutrient medium;
- determination of antibodies in blood serum (no less than a fourfold increase in antibody titers in paired sera taken in the acute stage of the disease and after 1–3 weeks);
- electroencephalogram and MRI (give nonspecific results and are only of relative importance for diagnosis).