Sumamed® (Sumamed®)
Antacids
Antacids do not affect the bioavailability of azithromycin, but reduce the maximum blood concentration by 30%, so the drug should be taken at least one hour before or two hours after taking these drugs and eating.
Cetirizine
Concomitant use of azithromycin with cetirizine (20 mg) for 5 days in healthy volunteers did not lead to pharmacokinetic interaction or a significant change in the QT interval.
Didanosine (dideoxyinosine)
The simultaneous use of azithromycin (1200 mg/day) and didanosine (400 mg/day) in 6 HIV-infected patients did not reveal changes in the pharmacokinetic indications of didanosine compared to the placebo group.
Digoxin (P-glycoprotein substrates)
Concomitant use of macrolide antibiotics, including azithromycin, with P-glycoprotein substrates, such as digoxin, leads to increased concentrations of P-glycoprotein substrate in the blood serum. Thus, with the simultaneous use of azithromycin and digoxin, it is necessary to take into account the possibility of increasing the concentration of digoxin in the blood serum.
Zidovudine
Concomitant use of azithromycin (single dose of 1000 mg and multiple doses of 1200 mg or 600 mg) has a minor effect on the pharmacokinetics, including renal excretion of zidovudine or its glucuronide metabolite. However, the use of azithromycin caused an increase in the concentration of phosphorylated zidovudine, a clinically active metabolite in peripheral blood mononuclear cells. The clinical significance of this fact is unclear.
Azithromycin interacts weakly with isoenzymes of the cytochrome P450 system. Azithromycin has not been shown to participate in pharmacokinetic interactions similar to erythromycin and other macrolides. Azithromycin is not an inhibitor or inducer of cytochrome P450 isoenzymes.
Ergot alkaloids
Given the theoretical possibility of ergotism, the simultaneous use of azithromycin with ergot alkaloid derivatives is not recommended.
Pharmacokinetic studies were conducted on the simultaneous use of azithromycin and drugs whose metabolism occurs with the participation of isoenzymes of the cytochrome P450 system.
Atorvastatin
Concomitant use of atorvastatin (10 mg daily) and azithromycin (500 mg daily) did not cause changes in atorvastatin plasma concentrations (based on an HMC-CoA reductase inhibition assay). However, in the post-marketing period, isolated case reports of rhabdomyolysis have been received in patients receiving concomitant azithromycin and statins.
Carbamazepine
Pharmacokinetic studies involving healthy volunteers did not reveal a significant effect on the plasma concentrations of carbamazepine and its active metabolite in patients receiving concomitant azithromycin.
Cimetidine
In pharmacokinetic studies of the effect of a single dose of cimetidine on the pharmacokinetics of azithromycin, no changes in the pharmacokinetics of azithromycin were detected when cimetidine was used 2 hours before azithromycin.
Indirect anticoagulants (coumarin derivatives)
In pharmacokinetic studies, azithromycin did not affect the anticoagulant effect of a single 15 mg dose of warfarin administered to healthy volunteers. Potentiation of the anticoagulant effect has been reported after simultaneous use of azithromycin and indirect anticoagulants (coumarin derivatives). Although a causal relationship has not been established, the need for frequent monitoring of prothrombin time should be considered when using azithromycin in patients receiving indirect oral anticoagulants (coumarin derivatives).
Cyclosporine
In a pharmacokinetic study involving healthy volunteers who took azithromycin (500 mg/day once) orally for 3 days and then cyclosporine (10 mg/kg/day once), a significant increase in maximum plasma concentration (Cmax) and area under the concentration-time curve (AUC0-5) of cyclosporine. Caution is advised when using these drugs together. If simultaneous use of these drugs is necessary, it is necessary to monitor the concentration of cyclosporine in the blood plasma and adjust the dose accordingly.
Efavirenz
Concomitant use of azithromycin (600 mg/day once) and efavirenz (400 mg/day) daily for 7 days did not cause any clinically significant pharmacokinetic interaction.
Fluconazole
Concomitant use of azithromycin (1200 mg once) did not change the pharmacokinetics of fluconazole (800 mg once). The total exposure and half-life of azithromycin did not change with simultaneous use of fluconazole, however, a decrease in Cmax of azithromycin was observed (by 18%), which had no clinical significance.
Indinavir
Concomitant use of azithromycin (1200 mg once) did not cause a statistically significant effect on the pharmacokinetics of indinavir (800 mg three times a day for 5 days).
Methylprednisolone
Azithromycin does not have a significant effect on the pharmacokinetics of methylprednisolone.
Nelfinavir
The simultaneous use of azithromycin (1200 mg) and nelfinavir (750 mg 3 times a day) causes an increase in the equilibrium concentrations of azithromycin in the blood serum. No clinically significant side effects were observed and no dose adjustment of azithromycin was required when used concomitantly with nelfinavir.
Rifabutin
The simultaneous use of azithromycin and rifabutin does not affect the concentration of each drug in the blood serum. Neutropenia has sometimes been observed with simultaneous use of azithromycin and rifabutin. Although neutropenia has been associated with the use of rifabutin, a causal relationship between the use of the combination of azithromycin and rifabutin and neutropenia has not been established.
Sildenafil
When used in healthy volunteers, there was no evidence of the effect of azithromycin (500 mg/day daily for 3 days) on the AUC and Cmax of sildenafil or its main circulating metabolite.
Terfenadine
In pharmacokinetic studies, there was no evidence of interaction between azithromycin and terfenadine. There have been isolated cases reported where the possibility of such an interaction could not be completely excluded, but there was no concrete evidence that such an interaction occurred.
It has been found that the simultaneous use of terfenadine and macrolides can cause arrhythmia and prolongation of the QT interval.
Theophylline
No interaction has been detected between azithromycin and theophylline.
Triazolam/midazolam
No significant changes in pharmacokinetic parameters were detected with simultaneous use of azithromycin with triazolam or midazolam in therapeutic doses.
Trimethoprim/sulfamethoxazole
Concomitant use of trimethoprim/sulfamethoxazole with azithromycin did not reveal a significant effect on Cmax, total exposure or renal excretion of trimethoprim or sulfamethoxazole. Azithromycin serum concentrations were consistent with those found in other studies.
Diagnosis and treatment of cystitis in children
23.07.2019
15803
1
| Mlynchik Elena Vyacheslavovna Candidate of Medical Sciences, pediatric urologist-andrologist, Center for Urology-Andrology and Pathology of the Pelvic Organs, Children's City Clinical Hospital No. 9 named after. G.N. Speransky, Moscow |
At the seminar “Urinary syndrome and pyeloectasia in children”, held within the walls of the Morozov Children’s Hospital, candidate of medical sciences, pediatric urologist-andrologist Elena Vyacheslavovna Mlynchik (Center for Urology-Andrology and Pathology of the Pelvic Organs of the Children’s City Clinical Hospital No. 9 named after G. N. Speransky, Moscow) spoke about approaches to the diagnosis and treatment of recurrent cystitis in children.
Features of cystitis in children
It is known that acute cystitis is easy to treat, in contrast, recurrent cystitis requires multi-stage therapy under dynamic control. Cystitis means inflammation of the mucous membrane and submucosal layer of the bladder, accompanied by disruption of its function. Statistics show that the disease occurs up to 6 times more often in girls than in boys.
Predisposing factors are disturbances in the urodynamics of the lower urinary tract, diseases of the external genitalia and pelvic organs, as well as a decrease in local immunological protection, violations of the integrity of the epithelial layer of the bladder as a result of exposure to various factors (cooling, trauma, surgery, stones, radiation, toxic substances ).
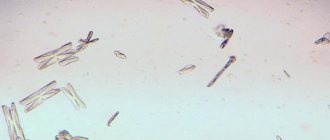
The most common causative agents of cystitis are E. coli (50–80% of cases), Klebsiella, Proteus, saprophytic staphylococcus, enterococci, Pseudomonas aeruginosa, as well as microbial associations (E. coli + focal streptococcus or epidermal staphylococcus, etc.). Cystitis is divided according to etiology into infectious and non-infectious, which, in turn, are divided into specific and nonspecific. By form - primary and secondary.
According to the flow - acute and chronic. According to the nature of the changes in the mucosa - catarrhal, cystic (bullous), granular, fibrinous, ulcerative, polypous, interstitial and necrotic cystitis are also distinguished. According to prevalence, focal (cervical, trigonitis) and diffuse cystitis are distinguished. The disease can occur with or without complications.
Algorithm for antibacterial therapy of acute and recurrent cystitis
1Cystitis in combination with abnormalities and/or obstruction of the urinary tract, urolithiasis, diabetes mellitus 2Do not use in regions with a high level of E. Coli resistance (>20%) to fluoroquinolones
Clinical picture and differential diagnosis
In all cases, especially in young children, it is necessary to carry out a differential diagnosis of acute cystitis with acute pyelonephritis. Thus, with cystitis, the temperature rarely rises above 38 degrees C, there may be no symptoms of intoxication and lower back pain, which are always observed in acute pyelonephritis. At the same time, dysuria is always present, often hematuria. Leukocyturia is often moderate, while with pyelonephritis it is moderate to severe. True bacteriuria is observed in both cases.
In some cases, differential diagnosis is required with neurogenic bladder dysfunction (normal urine tests and cultures, reduced bladder volume, especially when awake), vulvovaginitis, prostatitis and dysmetabolic nephropathy (oxaluria, uraturia). It is worth remembering, however, that these diseases can also accompany cystitis, which happens in approximately 40% of cases. In general, with chronic cystitis in children, exacerbations are not always accompanied by an increase in body temperature and symptoms of intoxication.
Asymptomatic leukocyturia and bacteriuria are often observed; dysuric phenomena may be absent. Urinary incontinence may occur. For diagnosis in the acute period, a urine test (general or Nechiporenko’s) is performed every 5–7 days, and a clinical blood test is also taken. In case of relapses, urine culture is performed for flora and sensitivity to antibiotics and uroseptics, as well as a biochemical study of urine. An ultrasound of the urinary system is prescribed to determine residual urine.
The rhythm of urination over two days is determined (urination diary). If possible and if necessary, uroflowmetry and cystourethroscopy are performed. If cystitis is prolonged, there is no effect of traditional therapy, there is a complicated medical history, or a suspected mixed infection, urine is tested for chlamydia, mycoplasma, ureaplasma, fungi, viruses and tuberculosis microbacteria (urine culture three times). Additional examination methods for chronic recurrent cystitis include cystourethrography, urodynamic studies, nephroscintigraphy, and studies of immune status.
If necessary, consultation with specialists is indicated: urologist, neurourologist, neurologist, phthisiatrician, gastroenterologist, proctologist, gynecologist and andrologist. Indications for cystoscopy include more than two episodes of acute cystitis, asymptomatic leukocyturia or bacteriuria, episodes of hematuria, and resistance to conventional therapy.
Features of treatment tactics
Treatment of acute cystitis should be aimed at eliminating pain, normalizing urination disorders, eliminating the pathogen and inflammation. Patients are prescribed therapeutic diet No. 5, a gentle diet with the exception of hot and spicy foods, spices and extractives, and a plentiful drinking regimen. In case of severe pain, antispasmodics are indicated, as well as sitz baths with solutions of antiseptic herbs. Thermal procedures and magnetic therapy can be prescribed locally. Antimicrobial therapy is prescribed for 7–10–14 days, depending on the patient’s condition.
Among uroseptics, furazidine is considered first-line therapy. If it is ineffective, pipemidic or nalidixic acid preparations, or fosfomycin are used once or twice. The second line of therapy is protected penicillins, amoxicillin/clavulanic acid, as well as 2, 3 and 4 generation cephalosporins. Once the symptoms subside, herbal medicine is prescribed. To prevent relapses, immunotherapy is recommended - the drug Uro-Vaxom, prescribed for 3 months.
Complications of cystitis include acute pyelonephritis, neurogenic bladder dysfunction, often accompanied by urinary incontinence, the formation of vesicoureteral reflux, and rarely - urethral stenosis and sclerosis of the bladder neck.
There are a number of basic principles for the treatment of recurrent cystitis:
- antibacterial therapy and uroantiseptics;
- according to indications - intravesical instillations for various forms of recurrent cystitis;
- various types of physiotherapy therapy;
- improvement of bladder circulation, restoration of bladder functions;
- treatment and prevention of vulvitis;
- normalization of colon function, exclusion of episodes of encopresis;
- according to indications - immunomodulatory therapy.
For catarrhal cystitis, alternating 10-day courses of uroseptics are prescribed for 1 month, for bullous cystitis - from 1 to 3 months, for fibrinous cystitis - at least 3 months. A maintenance dose of the drug can be prescribed for up to 6–12 months. Drug therapy may be prescribed to improve cystic circulation.
This category includes antihypoxants (succinic acid derivatives, cytochrome C), metabolite therapy (cocoments, group B drugs, carnitine), for neurogenic dysfunction - nootropics (gopanten, nicotinic acid derivatives), for severe detrusor hyperreflexia - M-cholinergic blockers (oxybutynin, trospium, tolterodine, bellataminal). These drugs have age restrictions and should be used under the control of residual urine.
For intravesical administration for bullous, bullous-fibrinous and fibrinous cystitis, a solution of dioxidin 0.5–1%, miramistin 0.01% or dioxidin 1% + aloe extract + novocaine 0.5% + hydrocortisone acetate, as well as hyaluronic acid preparations are used. For bullous and granular cystitis in the acute stage - derinat 0.25% or a solution of collargol 1:1000 - 1:100 or silver nitrate 1:5000 - 1:500 according to scheme No. 10.
Intravesical instillations are contraindicated in acute cystitis, catarrhal and hemorrhagic cystitis, as well as uninfected forms of bullous cystitis. They should be prescribed with caution for vesicoureteral reflux. Physiotherapy is carried out in courses 3-4 times a year. Paraffin and ozokerite applications, dry heat, and mud are prescribed. For catarrhal and bullous cystitis, magnetic therapy can be used.
For catarrhal and bullous bacterial cystitis - quantum (laser) therapy. In all cases, except for acute and hemorrhagic cystitis, TNF therapy can be prescribed. For any form of the disease - electrophoresis (zinc-iodine, hydrocortisone, methenamine). It is possible to use vibroacoustic effects (Vitafon device) and hyperbaric oxygenation. The main factors in treatment, as Elena Vyacheslavovna emphasized, are its phasing and regularity
Material prepared by Yu.G. Boldyreva, special. corr. Urology Digest The full version of the report can be viewed on Uro.TV
Topics and tags
Urology Digest
Comments
Kuleshova Yana Stanislavovna - 07.21.2020 - 15:37:33
The main thing in treating any disease is to identify it in time. Moreover, now there are safe examination methods. I regularly do ultrasounds. I know a very good place in Obolon where they do examinations very accurately https://medikom.ua/ru/uzi-kiev/. So, polycystic disease was detected in time even before it began to bother me. I started treatment on time = there was no surgery.
To post comments you must log in or register