Reception is strictly by appointment only!!!
Doctor Plus LLC License No. LO-77-01-004801 Treatment of anuria in the clinic +7 (495) 125-49-50
Make an appointment at the clinic
- +7 (495) 125-49-50
- Addresses of clinics in Moscow
- Daily
- call me back
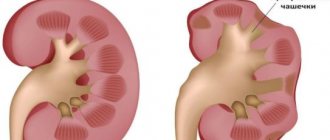
Anuria is a disease that is characterized by urine not entering the bladder and, as a result, not being excreted from it. This condition causes a significant reduction in urine output per day. This disease is characterized not only by a lack of fluid in the bladder, but also by the urge to go to the toilet. The disease is very similar to the symptom of acute urinary retention. However, these two conditions differ significantly from each other.
In acute urinary retention, the bladder is full and the person constantly has a strong desire to urinate. This condition means that there is a problem with urine output. Anuria is a more complex disease. Here the bladder is empty; it cannot fill with fluid due to the presence of pathology in the human kidneys. This condition is very dangerous and requires immediate medical intervention.
Clinical forms
The following types of anuria are distinguished.
Arenal anuria
observed with renal aplasia in newborns or as a consequence of erroneous removal of a single kidney.
Prerenal anuria
occurs more often as a result of insufficient blood flow to the kidneys (shock, heart failure) or its complete cessation (thrombosis of the aorta, inferior vena cava, renal arteries or veins), as well as as a result of hypohydration (blood loss, profuse diarrhea, uncontrollable vomiting).
Insufficient blood flow to the kidneys causes ischemia, which leads to necrosis of the tubular epithelium, and subsequently to the development of dystrophic changes in the renal parenchyma.
Renal anuria
(secretory) occurs as a result of significant damage to the renal parenchyma, which is based on anoxia due to various reasons (intoxication, poisoning with organic poisons, salts of heavy metals, etc.). Anoxia plays a major role in the pathogenesis of renal, as well as prerenal, forms of anuria. The difference between these types of anuria is that the prerenal form develops due to ischemia and circulatory anoxia, and the renal form develops due to histotoxic anoxia. Morphological and functional changes in the kidneys in prerenal and renal anuria are similar.
Subrenal anuria
(postrenal, excretory, obstructive) occurs as a result of a violation of the outflow of urine from the upper urinary tract. The most common cause of this is bilateral kidney stones, compression of the ureters by a tumor, and incorrect ligation of the ureters during surgery.
In addition to these types of anuria, some clinicians also distinguish between reflex-peripheral and reflex-renal anuria. Reflex-peripheral anuria occurs when irritants from various body systems act on completely healthy kidneys (for example, when the urethra is dilated, immersed in cold water, etc.). Reflex-renal anuria occurs reflexively due to the transfer of irritation from a diseased kidney during obstruction of its ureter to a healthy one (reno-renal reflex). The pathogenesis of the so-called reflex anuria is a violation of blood circulation in the kidney, therefore this type of anuria can be classified as prerenal.
There are also intoxication and traumatic anuria. Intoxication anuria is a consequence of severe general intoxication (for example, sepsis, intestinal obstruction, hepatorenal syndrome); may be prerenal or renal. Traumatic anuria is a manifestation of crush syndrome and is prerenal.
Causes of anuria
Often the causes of this clinical situation are due to improper functioning of the kidneys and ureters.
In addition, some diseases can result from urine not entering the bladder:
- stones in the kidneys. There are rare cases when this pathology becomes the cause of the disease. In order to prevent urine from completely entering the bladder, it is necessary to block two urinary canals at once. The resulting stones can block only one of the ureters;
- the presence of a tumor located near the bladder. When it grows and reaches a significant size, the paths for urine discharge are blocked;
- cardiovascular failure causes a condition in the body in which the kidneys cannot filter urine;
- severe form of alcohol or heavy metal poisoning;
- chronic kidney diseases.
If you have any problems with the kidneys, it is necessary to undergo regular examinations by a urologist in order to prevent the development of a more serious form of the disease. The patient can also use the service of calling a urologist at home.
You can make an appointment with a urologist from our consultants by calling +7 (495) 125-49-50
Prices for urologist services Addresses of clinics Ultrasound of the prostate Itching in the urethra Blood tests for PSA Calling a urologist to your home
Anuria
Anuria is the absence of urine in the bladder and urination.
It is necessary to distinguish anuria from acute urinary retention, in which the bladder is full of urine, but the act of urination is impossible due to obstruction of its outflow through the urethra (acute urinary retention).
With anuria, the bladder is empty. Urine is not excreted by the kidneys or does not enter the bladder due to compression or obstruction of the ureters.
Depending on the cause, secretory (prerenal, renal, arenal and reflex) and excretory (postrenal) anuria are distinguished.
What are the types of anuria?
Prerenal anuria occurs as a result of cessation of blood flow to the kidneys, i.e., in pathological conditions accompanied by a decrease in systolic blood pressure below 50 mm Hg. Art.
Causes:
- in acute heart failure;
- due to thrombosis or embolism of the renal vessels, thrombosis of the inferior vena cava;
- with dehydration (as a result of blood loss, diarrhea, uncontrollable vomiting or diarrhea);
- with heavy blood loss;
- as a result of shock (septic, hemorrhagic, painful, post-transfusion, allergic, etc.).
Renal anuria is caused by pathological processes in the kidney itself, leading to damage to the renal parenchyma (glomerular apparatus of the kidney).
Causes:
- in the late stages of chronic glomerulo- and pyelonephritis
- for polycystic disease, nephrotuberculosis and other kidney diseases,
- for sepsis,
- when transfusion of incompatible blood,
- for kidney damage and extensive burns
- in case of poisoning with poisons or drugs (poisoning with mercury, phosphorus, lead, acetic acid, salts of heavy metals, alcohol surrogates, sulfonamide drugs, antibiotics, etc.).
Arenal anuria is relatively rare. It is observed in newborns with congenital absence (aplasia) of the kidneys.
The absence of urine in newborns during the first 24 hours of life is not a pathology, whereas if urine is not excreted for a longer period of time, the condition is regarded as anuria and requires immediate diagnostic and therapeutic measures.
Reflex anuria (reflex-peripheral and reflex-renal) anuria occurs as a result of the inhibitory effect of the central nervous system on urination under the influence of various stimuli (surgery).
Postrenal anuria occurs when there is an obstruction to the outflow of urine from the kidneys, therefore this type of anuria is classified as excretory. It is most often found in urological practice. The main reason for its occurrence is ureteral stones or a ureteral stone in a single (or only functioning) kidney, as well as iatrogenic damage to the ureters (their ligation or suturing during surgical and gynecological operations on the pelvic organs).
Postrenal anuria can be caused by compression of the ureters by tumor tissues, scars or inflammatory infiltrate in the retroperitoneal tissue of the small pelvis (neoplasm of the uterus and its appendages in the late stages of the tumor process, metastases to the retroperitoneal lymph nodes, prostate and bladder cancer, rectal or sigmoid colon cancer, scar-sclerosing process after radiation therapy of the abdominal organs).
Symptoms of anuria
- Initially, the urge to urinate stops.
- After 1-3 days, signs of uremic intoxication appear, manifested by loss of appetite, dry mouth, ammonia odor from the mouth, thirst, nausea, vomiting, constipation, which, as uremia increases, are replaced by diarrhea.
- Symptoms of damage to the central nervous system gradually develop: asthenia, headache, muscle pain, drowsiness, sometimes agitation, delirium, as well as signs of pulmonary (shortness of breath) and cardiovascular failure (hypotension, bradycardia, arrhythmia).
- Peripheral edema is possible.
How is anuria treated?
Anuria is a condition that threatens the patient's life, requiring emergency medical care and urgent hospitalization. The totality of necessary therapeutic measures depends on the cause of anuria. Thus, in patients with prerenal and arenal forms of secretory anuria, emergency medical care should be aimed at maintaining cardiovascular activity.
In case of shock, efforts are made to restore normal blood pressure levels. In case of large blood loss, it is compensated and means are used to help stabilize central venous pressure.
In case of renal anuria, urgent hospitalization in a hospital is indicated, where hemodialysis or peritoneal dialysis can be performed.
For postrenal anuria, the main type of treatment is surgery, so such patients are advised to undergo urgent hospitalization in a urological or surgical department, where X-ray and ultrasound examinations can be performed and emergency care can be provided, including catheterization of the ureters, and if it is impossible to pass a ureteral catheter along the ureter above the obstacle, nephrostomy .
https://www.healthline.com/health/anuria https://studfiles.net/preview/5963477/page:3/
Symptoms of the disease
The most pronounced symptom is a significant reduction in urine excretion from the body or its complete absence.
There are other signs of this disease:
- fatigue that constantly increases;
- the appearance of swelling;
- vomiting, diarrhea;
- shortness of breath;
- constant desire to go to bed;
- pain in the lower back;
- bad breath;
- constant desire to drink;
- irritability of the patient, which can lead him to apathy.
This is not the entire list of symptoms, the presence of which indicates that urine is not entering the bladder.
Treatment
Treatment depends on the type, causes and manifestations of anuria. In case of subrenal anuria, the main measures are aimed at restoring the impaired passage of urine: catheterization of the ureters, early surgical intervention in the form of pyelonephrostomy (see Nephrostomy, Pyelostomy). In case of arenal, prerenal and renal forms of anuria, the patient should be treated in a renal center (see), equipped with equipment for dialysis (see Hemodialysis, Artificial kidney, Peritoneal dialysis).
If, with subrenal anuria, the patient’s condition is extremely severe due to uremic intoxication, then before surgery it is necessary to perform hemodialysis and then resort to pyelo- or nephrostomy. Considering the severity of the patient’s condition, the operation should be performed on the most functionally capable kidney (pain in the corresponding half of the lumbar region indicates the most functionally capable kidney).
With subrenal anuria, kidney function can be determined using radioisotope renography (see Radioisotope renography); the presence of a secretory segment of the curve indicates sufficient functional reserves of the organ. In prerenal, renal forms of anuria as a manifestation of acute or chronic renal failure, the main treatment is to restore the water-electrolyte balance to normal and eliminate hyperazotemia. For this purpose, detoxification therapy is used: intravenous administration of 10-20% glucose solution up to 500 ml, 200 ml of 2-3% sodium bicarbonate solution. With anuria, the patient should not be given a total of more than 700-800 ml of fluid per day, as this is dangerous due to the possibility of developing severe extracellular hyperhydration. The administration of these solutions should be combined with gastric lavage and siphon enemas.
For anuria caused by poisoning with mercury preparations, the use of unithiol is indicated (see). Unithiol is prescribed subcutaneously and intramuscularly, 1 ml of a 5% solution per 10 kg of weight, 3-4 injections on the first day, 2-3 on subsequent days.
All patients with acute renal failure should be treated in a kidney center, where extracorporeal dialysis machines can be used if necessary. Indications for the use of an “artificial kidney” for anuria are: electrolyte disturbances, especially hyperkalemia, hypercreatininemia, azotemia (urea content in the blood serum 300 mg% or higher), extracellular hyperhydration. The use of hemodialysis has significantly reduced deaths due to anuria. However, sometimes there is a need for a kidney transplant (see).
Prognosis for anuria
The most unfavorable prognosis is for sepsis in combination with acute renal failure and anuria. Mortality is close to 80% of cases.
In general, the prognosis for life with anuria depends on the restoration of the functional capacity of the kidneys, the reserve capabilities of the body, the presence of concomitant pathologies, the initial state of the genitourinary system, and the timeliness of medical care.
Victoria Mishina, urologist, medical columnist
7, total, today
( 40 votes, average: 4.58 out of 5)
Urinary tract infections: symptoms and treatment
Urinary incontinence in women: causes and treatment
Related Posts
Urine standards
Anuria can be calculated by diuresis. This is a certain volume of urine excreted by the kidneys per day. Norms range from 800 to 1500 ml. Any deviations beyond the lower limit indicate violations. A healthy person goes to the toilet 4-8 times a day (1 time at night). Rare cases of urination (2-3 times and a complete absence of urge) indicate problems with the kidneys.
Typically, anuria causes pain, and passing urine does not relieve the condition. It should not be confused with oliguria, when the amount of fluid excreted does not exceed 400 ml per day. The danger of anuria is the rapid development of complications that can lead to death.
Symptoms
Anuria has several manifestations, but patients report the same complaints. The final diagnosis is established only after laboratory and instrumental studies.
Signs:
- no urge to go to the toilet to urinate;
- severe renal failure;
- swelling throughout the body, often in the limbs;
- with kidney infections there is pain;
- thirst, lethargy, headaches, apathy;
- Deviations from the digestive, respiratory and nervous systems begin (convulsions, muscle spasms, cracked tongue, hiccups).
The final manifestation is renal coma and poisoning of the body. A critical state of anuria occurs on days 7-9.
Features in men and women
Anuria affects both male and female genders equally. The manifestations are no different, but in men the pain syndrome is more pronounced. When examining and palpating the groin, the patient may grimace or pull back his hand.
A large percentage of the development of pathology occurs in older people. And in the age group from 18 to 45 years, such cases are much less common.
Anuria in children
In children, as in adults, arenal, prerenal, renal and subrenal forms of anuria
, but mixed forms are more common.
Prerenal anuria
observed in acute gastrointestinal disorders, especially in infants. With uncontrollable vomiting and profuse diarrhea, water-electrolyte metabolism is disrupted, exicosis, hypovolemia develops, and the blood supply to the kidneys is disrupted. A similar condition can develop in a child in the summer at high temperatures, excessive sweating and insufficient fluid intake. This should also include cases of physiological anuria in newborns, when on the first day after birth the child has no urine output due to an insufficient amount of fluid received or a large loss of it with feces. In infants, anuria can develop due to hemolytic disease of the newborn. In this disease, anuria develops against the background of hemolytic anemia and thrombocytopenia. If anuria lasts from several days to two weeks, the prognosis is serious.
Renal anuria in young children
occurs with acute thrombosis of the renal veins, acute hemorrhagic cortical necrosis of the kidneys, with damage to the tubular apparatus of the kidneys, and with various poisonings.
In older children, renal anuria is observed in diffuse pathological processes in the kidneys (glomerulonephritis, acute tubulonecrosis and others). With diffuse glomerulonephritis, the anuric phase develops in the first week of the disease and is eliminated with proper treatment within a few days.