General characteristics and possible causes in men and women
Excessive physical activity, frequent stress, poor nutrition - all these are considered to be the causes of flatulence and urination problems.
If the number of urinations is more than 12 times per day, and it is accompanied by gases, a deviation from the normal functioning of the genitourinary system is suspected. Frequent urination in women is caused by many different reasons. If a person drinks a lot of liquid, this directly affects the frequency of emptying the bladder. During pregnancy, women may experience flatulence and the frequency of urges increases due to the fact that the fetus puts pressure on the genitourinary organs. If pain occurs when urinating, this indicates the onset of an inflammatory process in the bladder or cystitis.
In men, constant gas and frequent urination are sometimes caused by a disease such as hemorrhoids. These symptoms are dangerous with hemorrhoids, since the condition is aggravated due to increased pressure on the cavernous vessels. Gas can also be caused by cancer. The patient's complaints about frequent urination and flatulence serve as a signal for the doctor to prescribe sigmoidoscopy of the rectum.
If you experience gas, bloating, flatulence, or frequent urination, it is recommended to visit a doctor for consultation. There is no specific diagnosis for flatulence, but the doctor will definitely prescribe several research methods to exclude other diseases. First of all, it is recommended to take urine, blood and feces for a general analysis. A blood test is done to check for celiac disease. Then an ultrasound examination of the abdominal cavity is prescribed to exclude the development of a tumor. Sigmoidoscopy and colonoscopy are indicated.
A correct lifestyle, proper nutrition and diet will quickly bring the intestines and bladder back to normal, if no serious pathologies are detected with symptoms such as frequent urination and flatulence. The diet must be selected individually for each patient, depending on the symptoms of the disease and the body’s reaction to certain types of food. It is recommended to keep a diary where you write down all the types of foods you eat. This will help to track the body’s reaction to certain types of foods and select the appropriate menu.
To restore the condition of the bladder, herbal medicine is used: for women - douching with chamomile decoctions and other herbs, for men - rinsing the penis. It is recommended to control the amount of liquid consumed - it should not be too much. Some situations with frequent urination and flatulence require traditional medical treatment. In such cases, the following medications are prescribed:
- antispasmodics and laxatives;
- antidiarrheals;
- antidepressants;
- anti-inflammatory medications.
Treatment is prescribed aimed at restoring bladder function and getting rid of flatulence using folk and traditional methods
It is recommended to take probiotics - nutritional supplements that help restore intestinal microflora. Reducing stressful situations and increasing stress tolerance reduces the risk of a new exacerbation of symptoms. You can use relaxation exercises, such as meditation. Playing sports and regular exercise (running, walking) will help strengthen muscles and strengthen the body's immune system, which is an excellent preventative effect.
Problems such as bloating and frequent urination, at first glance, may not be related to each other. But if you take a closer look at each of the problems separately, you will be able to see this thin thread connecting flatulence and the feeling of a full bladder. Observing such phenomena frequently, the patient should not wait until they pass on their own; at the first opportunity, one should consult a doctor to find out the root cause of gas formation during urination and determine the subsequent plan of therapeutic action.
Gas formation is a normal physiological process that occurs in the intestines. Eating certain foods, having an unhealthy diet, or drinking carbonated drinks will cause increased gas formation. The following symptoms accompany this pathological condition:
- stomach ache;
- specific smell of air emitted from the rectum;
- stool disorders;
- bloating;
- nausea;
- rumbling in the abdominal cavity;
- general malaise;
- burning pain in the heart muscle;
- frequent belching;
- heart rate fluctuations;
- worsening mood.
As for urination, the volume and frequency of fluid released is individual, as it depends on many factors (metabolic intensity, physiological characteristics of the human body, drinking regime). However, people often notice that the urge to go to the toilet has become more frequent and, moreover, has become accompanied by discomfort, pain and flatulence. In this case, the patient should consult a doctor.
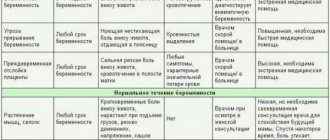
Pathology of peri- and postmenopause
The share of postmenopausal osteoporosis among all forms of osteoporosis is 85%. The incidence of postmenopausal osteoporosis in developed countries among white women is 25-40%. Densitometric examination in accordance with WHO criteria revealed osteoporosis in 30.5-33.1% of women aged 50 years and older. The social significance of osteoporosis is determined by its consequences - fractures of the vertebrae and bones of the peripheral skeleton, which leads to an increase in morbidity, disability and mortality among older women. Among the urban population of Russia, 24% of women aged 50 years and older have at least one clinically significant fracture. In Russia, the annual incidence of fractures of the distal forearm in women over 50 years of age is 563.8 per 100,000 population of the same age, and of the proximal femur - 122.5 per 100,000. It is assumed that an increase in the life expectancy of women up to 80 years will lead to an increase the incidence of femoral neck fractures to 6.25/million in 2050 and will exceed the 1990 indicators (1.66/million) by more than 3 times.PREVENTION
The goal of preventing osteoporosis is to maintain bone density and prevent fractures. Primary prevention is aimed at creating and maintaining skeletal strength during various periods of a woman’s life (during the period of intensive growth and formation of peak bone mass, during pregnancy and lactation, and in the postmenopausal period).
Primary prevention includes:
- Healthy diet (foods high in calcium, avoiding excess protein intake).
- Active lifestyle and regular exercise.
- Maintaining optimal body weight.
- Adequate intake of calcium (up to 1000 mg/day) and vitamin D (400 IU/day) starting in early childhood.
- Providing the body with calcium during pregnancy and lactation (1200 mg/day).
- Providing the body with calcium (1000 mg/day) and vitamin D (800 IU/day) in peri and postmenopause.
- A healthy lifestyle (excluding smoking, alcohol consumption, coffee abuse, fasting and unbalanced diet).
- Adequate sun exposure.
Secondary prevention is aimed at preventing fractures in cases of already developed osteoporosis:
- Use of adequate doses of calcium and vitamin D supplements.
- Correction of estrogen deficiency conditions (amenorrhea, surgical and natural menopause, chemotherapy, radiation therapy to the pelvic area) using HRT as the first line of prevention of postmenopausal osteoporosis.
- The use of non-hormonal drug therapy for osteoporosis.
- Prevention of falls.
- Use of hip protectors and corsets.
- Correction of conditions and diseases that increase the risk of falls.
- Treatment of conditions that negatively affect bone metabolism.
- A healthy lifestyle, including moderate physical activity, a balanced diet, and the elimination of bad habits.
SCREENING
Key indicators for screening:
- age,
- presence of risk factors for fractures,
- history of fractures.
Dual-energy X-ray absorptiometry, or densitometry, evaluates bone health in the most important areas of the skeleton: the lumbar spine, proximal femur, and distal radius. It is used for screening and can detect a decrease in bone mineral density of 1-2%.
Indications for dual-energy X-ray absorptiometry:
- Women aged 65 years and older.
- Postmenopausal women under 65 years of age with risk factors.
- Fractures with minimal history of trauma.
- Diseases or conditions that lead to decreased bone mass.
- Taking medications that reduce bone mass.
CLASSIFICATION
There are primary (85%) and secondary (15%) osteoporosis.
Postmenopausal osteoporosis refers to primary osteoporosis (type I).
Primary osteoporosis:
- postmenopausal (type I);
- senile (type II);
- juvenile;
- idiopathic.
Secondary osteoporosis occurs against the background of the following conditions:
- endocrine diseases (hyperthyroidism, hyperparathyroidism, hypercortisolism, hypogonadism);
- gastrointestinal diseases, in which calcium absorption in the intestines decreases;
- long-term immobilization;
- chronic renal failure;
- diseases of the hematopoietic system;
- iatrogenic causes (long-term use of glucocorticoids, heparin, anticonvulsants, GnRH agonists);
- bad habits (alcohol abuse, coffee, smoking).
ETIOLOGY
Postmenopausal osteoporosis is a multifactorial disease. It is based on progressive bone loss that begins after menopause.
Risk factors for osteoporosis:
Unmodifiable:
- low bone mineral density;
- female;
- age over 65 years;
- Caucasian race;
- family history of osteoporosis and fractures with minimal trauma in relatives (mother, father, sisters) over the age of 50 years;
- hypogonadism;
- systemic use of glucocorticoids for more than three months;
- previous fractures;
- immobilization.
Modifiable risk factors:
- smoking;
- low physical activity;
- tendency to fall;
- insufficient calcium intake;
- vitamin D deficiency;
- alcohol abuse.
PATHOGENESIS
The mechanisms of the influence of sex hormones on bone tissue are not fully understood. However, it is known that these hormones, along with physical activity and good nutrition, are among the main factors determining the mass and quality of bone tissue. The role of sex hormones and their deficiency is especially important during puberty, reproductive and menopausal periods. During puberty, the production of sex hormones increases and the skeleton becomes the target of their action. Features of skeletal formation largely depend on the predominance of female or male sex hormones. Activation of bone metabolism manifests itself in a progressive increase in bone mass. Peak bone mass is reached between 20 and 30 years of age. Preservation of three main protective factors - physical activity, good nutrition and sufficient production of sex hormones - is a necessary condition for healthy aging of bone tissue, which begins after 40-45 years. In the first 5-10 years of natural menopause, there is a gradual decrease in the secretion of sex hormones. A decrease in estrogen levels leads to an acceleration of bone turnover and loss of bone matter (up to 3-5%/g). Peak bone mineral density and the rate of bone loss determine the risk of developing osteoporosis.
A drop in estrogen levels leads to an acceleration of bone metabolism due to increased resorption processes, which leads to a decrease in bone mineral density. Estrogens play a key role in the regulation of bone turnover, but the determining factors in this process are genetic.
CLINICAL PICTURE
The clinical picture of osteoporosis is quite poor, and in 1/2 of women it can be asymptomatic and clinically manifest as a fracture that occurs after a minor injury. The main complaints (regardless of the duration of menopause): pain in the sacrum and lumbar region that increases with physical activity and walking, general weakness, increased fatigue. Patients often indicate a feeling of heaviness between the shoulder blades and the need to rest during the day in a lying position. The pain syndrome intensifies as the disease progresses. Intense pain that does not stop with rest appears in the spine, pelvic area, and tibia. Often the cause of a sharp increase in pain is trabecular microfractures that occur after heavy lifting or awkward movement. The most common fractures are the thoracic and lumbar vertebrae, the distal radius, the ankles, and the proximal femur. As the disease progresses, deformation of the vertebral bodies occurs, muscle weakness increases, and posture is disrupted (kyphosis of the thoracic spine is formed). Vertebral fractures are accompanied by a decrease in height, decreased ability to work and the ability to self-care. Osteoporosis should be suspected if height decreases by more than 2 cm/year or 4 cm over a lifetime.
Studying the anamnesis is based on identifying risk factors for osteoporosis. Facts that may indicate osteoporosis:
- Decrease in height by more than 4 cm during life.
- Fractures with minimal history of trauma. (A minimal trauma fracture is defined as one that occurs spontaneously or from a fall from a height no higher than the person's own height, including fractures caused by coughing, sneezing, sudden movement, or lifting.)
- Chronic pain in the lumbar and thoracic spine, intensifying after physical activity or heavy lifting; bone pain.
- Kyphosis of the thoracic spine.
- Body mass index less than 19 (or body weight less than 57.7 kg).
- Estrogen deficiency conditions (amenorrhea, surgical and natural menopause).
The presence of causes leading to the development of secondary osteoporosis (taking drugs that affect bone metabolism; prolonged immobilization; diseases of the gastrointestinal tract).
What causes flatulence when urinating?
When the number of urinations is more than 12 times a day, and there is bloating of the intestines due to the accumulation of excess gases in it, then the normal functioning of the genitourinary system is probably impaired.
Flatulence is often observed when urinating in women in a position where the descending fetus in the womb puts pressure on the bladder and intestines. As a result, colic occurs, increased gas production and increased urination. In men, strong gases and a frequent desire to empty the bladder are often symptoms of hemorrhoids and its accompanying disease - prostatitis, which occurs due to the penetration of putrefactive bacteria from inflamed hemorrhoids into the prostate. The main symptom of prostatitis is frequent urination.
Often it is flatulence, as a symptom of many pathologies, in particular hemorrhoids, that is the reason for the constant desire to empty the bladder. This is due to the fact that in order to normalize stool, the patient is recommended to drink a large amount of liquid, so the urge to urinate in this case is normal.
Gas and frequent urination are 2 problems, to eliminate which you should know what caused them to appear. To do this, you will need to contact a specialized specialist who, through a diagnostic examination, will identify the main problem. The doctor will need data from instrumental and laboratory examinations. To rule out oncology, the doctor will write the patient a referral for sigmoidoscopy. This study consists of a complete examination of the rectum, allowing one to evaluate the clinical picture of the mucous membrane.
To get rid of flatulence, the patient should reconsider his diet and exclude from it foods that can increase gas formation (carbonated drinks, beans, sweet foods, flour products, vegetables). The diet is selected individually for each patient, depending on the body’s reaction to certain foods.
In order for the number of urinations to be normal, it will be necessary to restore the previous state of the bladder. Folk remedies, namely herbal medicine, will help with this. Women are prescribed douching, and men are prescribed rinsing the genitals with chamomile infusions and other medicinal herbs. In this case, you should reduce the amount of fluid consumed per day. If flatulence continues to accompany urination, then herbal medicine alone may not be enough and then doctors recommend taking pharmaceutical drugs. The patient may be prescribed antidepressants, antispasmodics, laxatives, anti-inflammatory and antidiarrheal drugs.
Patients are also prescribed probiotics, which are necessary to restore intestinal microflora. To avoid having to deal with the problem of gas formation and frequent urination again, doctors recommend increasing the body’s defenses, because only a strong immune system can cope with pathogenic microorganisms entering the body from the outside.
Renal colic is a symptom of an advanced stage of urolithiasis. People who have ever experienced it forever remember the severity of its manifestation. Sharp pain is not relieved by conventional medications (analgesics). Only after the administration of narcotic drugs can the pain be temporarily eliminated. However, this approach does not eliminate kidney disease.
Renal colic is caused by blockage of the urinary tract with a large stone, which makes it difficult for urine to pass out. As a result, urine accumulates in the renal pelvis and bladder, causing excessive distension of these organs.
Since the wall of the bladder is “saturated” with pain receptors, you can count on severe pain until the cause of the pathology, the urinary tract stone, is eliminated.