05/10/2021 | Category: Symptoms of cervical osteochondrosis
Many who had an ultrasound of the neck saw in the conclusion the phrase “impaired venous outflow.” Let us immediately note that if this is discovered, this is already good, it means that the doctor looked carefully, not in a hurry, and did not miss anything. Sometimes there is no such record, although in fact there is a problem. The lack of recording may be due to various reasons, including due to outdated equipment; we will not dwell on this, but further we will describe the factors and symptoms by which it can be understood that the venous outflow is impaired, even if this is not indicated by the ultrasound results.
What is a venous outflow disorder?
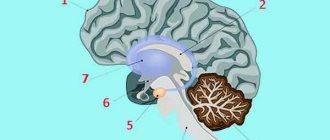
First of all, let's understand the anatomy. Imagine a spine. Veins run next to it, through which blood should flow freely from the head down. If the vertebrae are displaced, then the veins can be pinched, deformed, and because of this their capacity is reduced. Blood accumulates in the posterior cranial fossa.
With normal intracranial pressure, there is no outflow of blood through the compressed vessels. In order for the outflow to be restored, the blood must flow with greater pressure, that is, the pressure must increase. We all know that increasing blood pressure is not beneficial for the body, to put it mildly, and here it is a necessary measure to restore blood circulation, otherwise more serious problems will arise.
In the long term, stagnation of blood and impaired circulation in the brain are fraught with many bad consequences, but there is no need to be afraid. The human body is excellent at recovering on its own, plus it informs in advance about possible problems with unpleasant and even painful sensations. Therefore, you need to listen to your body and simply help it be healthy, which is not difficult to do.
After an increase in pressure, a sharp outflow occurs through the posterior or jugular veins. Changes in the condition of the jugular veins are easier to see on an ultrasound than changes in the vessels near the spine, on the back of the neck.
Helpful advice
When you go for an ultrasound, be sure to ask to look at the jugular veins. If they write to you that they are dilated, this is an accurate sign of venous stagnation and circulatory disorders in the brain.
Reference. It is more difficult to see a similar sign of a disorder in the spine. Therefore, it may be that the problem is already there, but it is not yet visible when examining the back of the neck.
The jugular veins dilate and lose elasticity when large volumes of blood are dumped through them. As a result, blood circulation worsens even more, and the body signals this with pain.
Degrees of venous stagnation
Venous congestion is not a separate disease. This is a complex disorder of the blood vessels, in which the normal flow of arterial blood to any organ (brain, lungs, lower and upper extremities) is maintained, but from this organ is disrupted
The degree of venous stagnation is determined by the depth of disorders associated with venous blood stagnation. However, since venous congestion can have many causes, it can be quite difficult to clearly determine the stage of venous congestion.
In the vast majority of cases, disturbances in the outflow of venous blood are caused by : - a physical obstruction inside the vein (thromtosis in thrombosis, cholesterol plaque in atherosclerosis); — excessive extensibility of the venous walls in varicose veins; - high intravenous pressure in cardiovascular diseases; — congenital underdevelopment of veins with venous dysplasia; - stagnation of lymphatic fluid in soft tissues during lymphostasis.
All these diseases lead to venous stagnation , but differ in clinical course and rate of development. That is why the degrees of venous stagnation are characteristics of a particular disease.
For example, in the case of varicose veins of the lower extremities, three phases of venous stagnation . 1. Compensatory phase . The patient experiences mild discomfort and suffers from increased leg fatigue. At this stage of varicose veins, the veins are still coping with the evacuation of blood from the legs. 2. Subcompensatory phase . The patient complains of swelling that occurs in the evening and disappears in the morning. Individual dilated veins may appear on the skin. At this stage of varicose veins, the venous walls gradually stretch, and the valves of the vessels begin to allow some of the blood back into the superficial veins. 3. Decompensatory phase . The patient complains of persistent swelling and severe pain in the legs. a network of varicose vessels appears on the skin and trophic ulcers may appear. At this stage of varicose veins, the veins practically lose the ability to independently lift blood from the legs to the heart, providing venous outflow.
Treatment of venous stagnation in varicose veins depends on the phase of the disease. So, in the first phase of the disease, to prevent the disease, it is enough to regularly wear compression hosiery “Intex” (15-18 mm Hg).
In the second phase of varicose veins, complex treatment is required, including taking medications, manual and hardware massage, physiotherapy and wearing Intex elastic underwear of a higher compression class 1 (18-22 mm Hg).
In the third phase, varicose veins most often require surgical intervention. Since even after surgery the risk of re-development of varicose veins remains high, people suffering from severe varicose veins have to wear Intex compression hosiery of a higher, 2nd compression class (23-32 mm Hg) all their lives.
Symptoms of impaired venous outflow
Headache
The most common symptom is pain due to increased intracranial pressure. The blood does not leave the head on time, and new portions of it continue to flow - the pressure rises, the body signals this with a headache.
A case from the practice of Dr. Shishonin
The man was diagnosed with migraine and prescribed medication. The patient took the pills with discipline, but there was no noticeable improvement. Migraine attacks did not become less frequent and were often as severe as before starting to take the drugs. The attack was very difficult to relieve with analgesics; you had to take the maximum allowable doses, and even they did not always work. The pain went away on its own after some time.
Dr. Shishonin recommended going for an ultrasound under the compulsory medical insurance policy and asking to look at the jugular veins. An ultrasound showed that they were dilated. The cause of the migraine became clear - increased intracranial pressure.
After conservative non-drug treatment, improvement occurred within two months.
Extreme migraine
A very painful symptom occurs due to loss of elasticity of the jugular veins. Up to a certain point they can withstand the increased load, and then they can no longer cope. Swelling appears in the brain stem. They are not yet dangerous to human life and health, but they cause severe pain in the ternary nerve.
This is an extreme degree of migraine, it is almost impossible to tolerate and difficult to relieve with analgesics. A person becomes incapacitated, no matter how strong his will is. In addition, nausea occurs, the patient is physically unable to drink liquids or eat food. A migraine can last a day and goes away on its own when the pressure rises to such an extent that blood discharge does occur. If such conditions are repeated frequently, it becomes potentially dangerous.
Ptosis of the eyelid
A case from the practice of Dr. Shishonin
The person suddenly developed ptosis and the mobility of the eyelid was impaired. The hospital carried out a full examination - a microstroke was not confirmed, and no tumor was found.
An ultrasound scan examined the veins in the neck and revealed gross venous congestion. Conservative treatment without pills gave results after six months. If a person had paid attention to the headaches that he often had earlier, the problem could have been solved faster.
Labored breathing
This symptom itself is ambiguous; there can be many reasons. But if it is accompanied by regular pain in the back of the head or temples, then the cause is most likely venous stagnation.
Lack of air due to a violation of venous outflow can occur either unexpectedly and without cause (not during physical activity, not in a stuffy room), or, as they say, out of the blue - during a walk, in a well-ventilated room. If such situations recur, and under different conditions, you need to check and treat the neck first.
What else you need to know about symptoms
There are many signs of circulatory problems. Any discomfort in the head, neck, chest, or upper back may indicate this problem. You need to undergo an examination, and in any case it will be useful to do simple exercises. Unlike pills, carefully performed gymnastics and gentle self-massage have no side effects, that is, in any case the condition will not worsen.
The main principle of the doctor is Primum non nocere (“First of all, do no harm”). Therefore, Dr. Shishonin recommends making maximum use of the natural recovery abilities inherent in our body.
Chronic venous insufficiency!
Selection of the optimal drug for pharmacotherapy of chronic venous insufficiency.
The article provides a review of literature data on the effectiveness and safety of modern pharmacotherapy for chronic venous insufficiency.
Chronic venous insufficiency (hereinafter referred to as CVI)
is one of the most common vascular pathologies. Currently, more than 35 million people suffer from it in Russia. Moreover, 15% of them have a decompensated form of venous insufficiency with trophic skin disorders and recurrent ulcers. The most common targets of CVI are women; Experts also note with concern the rejuvenation of such pathologies. The high prevalence of the disease, frequent relapses, and a large number of complications that provoke loss of ability to work and disability of patients lead to the need to search for new drugs for this category of patients. Until recently, little attention was paid to the pharmacotherapy of chronic venous insufficiency; treatment was carried out according to the scheme “surgery - sclerotherapy - compression treatment”.
Today, most patients receive conservative treatment and only 10-15% of patients with CVI are sent for surgery. Moreover, a significant proportion of patients who require surgical intervention during preparation for surgery and postoperative rehabilitation receive pharmacotherapy.
Groups of venotonics
For the pharmacotherapy of venous insufficiency, characterized by a pathological increase in the lumen of the veins and impaired circulation in the affected area, venotonics are used. Based on the chemical nature of the main active ingredients, the following groups of
venotonics
:
1. Venotonics based on flavonoids
- diosmin and hesperidin.
The drugs have a systemic effect and are intended for oral administration (Detralex, Venarus, Phlebodia 600, Vazoket, Diovenor 600, Neodisven Maximum). 2. Pharmaceutical preparations containing a synthetic analogue of the flavonoid rutin
-
troxerutin
(Troxevasin, Troxevenol).
This is the most “ancient” group. Includes both oral medications and dosage forms intended for topical use. 3. Medicines based on pentoxifylline.
They increase the tone of venous vessels by reducing capillary permeability.
Significantly improve tissue trophism. Unlike the above groups of drugs, they have serious contraindications and side effects are more common. 4. Preparations from medicinal raw materials
(phytotablets, as well as creams, ointments containing extracts and oils).
The modern pharmaceutical market offers venotonic drugs in various release forms. For CVI, as a rule, a course of venotonics is prescribed - 1-2 times a year for 2-3 months. The use of venotonics during pregnancy The
use of venotonics during pregnancy is especially important, when the load on the venous network increases sharply, body weight increases and complex hormonal changes in the body occur. Violation of venous outflow often becomes a companion to pregnancy and is accompanied by swelling of the lower extremities, a feeling of heaviness in the legs, and often attacks of acute hemorrhoids. If the symptoms of impaired venous outflow cause serious concern, you should contact a specialist who will select the correct treatment tactics. In the first trimester of pregnancy, when the fetus is especially sensitive to any influences, doctors recommend exclusively local use of venotonics (creams, gels, balms).
hesperidin- based venotonics can be used
and
diosmina
. It should be noted that to prevent damage to both arterial and venous vessels, venotonics should be prescribed as early as possible. This is especially true for diseases in which vascular changes lead to the development of damage to organs and systems of the entire body (diabetes mellitus, coronary heart disease, disorders of the blood coagulation system).
Neodisven Maximum
A survey of pharmacy visitors showed that most of them are ready to buy new drugs because they are more effective.
In this regard, the appearance on the pharmaceutical market of Neodisven Maximum
, a venotonic and angioprotective agent from the Russian-German company Erzig, is especially relevant. The drug is available in tablets and consists of diosmin and hesperidin in a ratio of 9:1. The use of the product reduces the distensibility of veins and venous stagnation, reduces capillary permeability and increases their resistance. At the same time, lymphatic drainage and blood microcirculation improve, the adhesion of leukocytes to the venous wall and their migration into paravenous tissues decreases, and a pronounced anti-inflammatory effect is observed. Blocks the production of free radicals, the synthesis of prostaglandins and thromboxane.
Research results confirm the activity of Neodisven aximum
in relation to indicators of venous hemodynamics. The maximum was demonstrated for the following parameters: venous capacity, venous distensibility, venous emptying time. Thus, the main principle of treatment for CVI is periodic courses of medications; standard therapeutic dosages are most often used. In this case, there is no need to prescribe several phlebotonics at once, since the polyvalent mechanism of action of most modern drugs makes it possible to carry out monotherapy.
Buy NEODYSVEN MAXIMUM
Dietary supplement NOT A MEDICINE.
* Baeva N.V. Selection of the optimal drug for pharmacotherapy of chronic venous insufficiency // Innovative development of science and education: collection of articles of the VIII International Scientific and Practical Conference. — ICNS “Science and Enlightenment.” — 2019.
How can you help yourself without pills?
There are two simple ways. The first can be used by each person independently without preparation. The second one is a little more difficult, but regular viewers and readers of Dr. Shishonin will master it very quickly.
It is better to use both methods: working on the points on the sides of the front of the neck, and working under the back of the head. This way, you will not only get rid of headaches and other symptoms of impaired venous outflow, but you will also feel more energetic, your mood and memory will improve. The main thing is to regularly devote time to yourself and help your body recover. The capabilities of the human body are almost limitless, but you need to develop them by doing gymnastics and self-massage.
Venous discirculation in childhood and adolescence
Introduction
Vascular lesions of the nervous system are an important problem in modern clinical neurology.
The study of cerebral venous circulation disorders remains one of the urgent tasks of modern medicine. The improvement of ultrasound equipment, as well as its software, has led to the fact that when studying blood flow in the arteries of the brain, it is possible to assess the state of venous blood flow at a fairly good level.
However, the main problem is that the data on the normative values of velocities in the venous system of the brain are extremely scattered, fragmentary and not always unambiguous.
In this regard, you often have to rely on your own experience, taking as a basis data from a number of literary sources (Table 1), which are more consistent with the features of this device, the quality of the resulting image and the age of the patient. The small number of ultrasound studies, which would contain data on the state of venous blood flow at the extra- and even more so at the intracranial levels, is explained primarily by hardware features, and only then by the insufficient amount of information on this issue in the periodical literature, the complexity of the spatial-anatomical three-dimensional perception of the intracranial venous system by diagnosticians, low need for such studies on the part of neurologists. Table 1
. Blood flow indicators (Vmax, cm/s) in the internal jugular veins and in the main intracranial veins/sines of the brain.
| Author | Internal jugular vein | Middle cerebral vein | Vienna Rosenthal | Vienna Galena | Direct sine | Internal cerebral vein | Vertebral veins |
| V.G. Lelyuk, S.E. Lelyuk, 2003 [1] | 7-45 right\ 12-33 left | 9 | 11 | 15 | |||
| J. Valdueza et al., 1996 [2] | 6-18 | 4-17 | |||||
| BG Schoser, 1999 [3] | 5-12 | ||||||
| E. Stolz et al., 1997 [4] | 13,8 ± 8,9 | 13,7 ± 4,7 | 31,7 ±15,6 | ||||
| R. Baumgartner et al., 1997 [5] | 4-15 | 7-19 | 12-39 | 10-18 | |||
| R. Aaslid, 1991 [6] | 23 ± 3 | ||||||
| V.A. Shakhnovich, 1998 [7] | 14-28 | ||||||
| M.L. Dicheskul et al., 2008 [8] | 9,8-20,9 | ||||||
| G.A. Ivanichev, G.B. Dolgikh, 2007 [9] | 22,0 ± 4,6* 20,1 ± 3,2** | 17,7 ± 3,3* 16,2 ± 2,2** | |||||
| G.B. Dolgikh, G.A. Ivanichev, 2008 [10] | 13,6 ± 0,3 | 23,4 ± 0,9 | 18,7 ± 0,9 |
Note. * - in children aged 1-12 months; ** - in children aged 1-3 years.
The purpose of this study was to assess correlation dependencies in patients with signs of venous discirculation at the intra- and extracranial levels, cerebral venous hemodynamics in children and adolescents with a clinical picture of “cranialgia”, with clarification of the cause-and-effect relationships that determine the formation of venous discirculation.
Material and methods
The study included 106 children aged from 2 to 18 years, average age 9.87 ± 3.9 years (from 2 to 6 years - 18 people, average age 3.8 ± 1.43 years; from 7 to 18 years - 88 people, average age 11.1 ± 2.99 years), sent for examination to the diagnostic center of Kaliningrad with a headache clinic or symptoms of vertebrobasilar insufficiency. During the examination, signs of dysgemia at the intra- and extracranial levels were identified in all of them. Doppler ultrasound studies of arterial and venous blood flow at the level of the neck and base of the brain were performed on a Medison Accuvix V10 device (South Korea), in B-, C-, PW-modes, linear (L5-12 MHz) and sector phased (P2- 4 MHz) sensors. Correlation dependencies were assessed between 94 clinical and instrumental indicators.
results
As a result of the study, it was found that discirculation in the vertebral vein (PV) system, as a rule, is a consequence of pronounced extravasal influences (vascular compression) on blood flow in the internal jugular vein (IJV) on the side of registration of dyshemia (r = + 0.67; p 0.05).
Dysgemia in the vein of Galen on the right is often accompanied by an increase in the tone of the VA, ICA and MCA on the ipsilateral side (as a consequence of reflex changes), just as the former is associated with kinks and S-shaped tortuosity of the ICA on the right. The effect of ICA tortuosity on venous outflow may be due to extravasal compression of venous vessels by tortuous arterial trunks with significantly higher intravascular pressure in the places of their closest abutment.
The relationship between “headache syndrome” and accelerated venous blood flow through the veins of Galen turned out to be extremely low (r = +0.22; p
In addition, a fairly clear picture of pronounced unilateral disturbances of both arterial blood flow and venous outflow was noted, which is probably due to the unity of the autonomic innervation of the arteriovenous system “head-neck”, the presence of complex compensatory mechanisms (reflex), as well as the indirect influence of the tone of the striated muscles neck and cervical spine, which is confirmed in a number of studies.
Discussion
From our own experience of working with devices from leading manufacturers of ultrasound equipment, it should be admitted that the best quality images of the cerebral venous network were often obtained using Medison Acuvix devices. At the same time, the images were of high quality in both C and PW modes, with a minimum of artifacts and interference.
Assessment of venous blood flow at the extracranial level (jugular veins, vertebral veins) causes fewer difficulties and is available on almost any device, except, perhaps, assessment of blood flow through the vertebral veins in persons with excess body weight, widespread osteochondrosis and a short neck, when even visualization vertebral arteries is carried out with great difficulty.
The structure of the cerebral venous system is presented in Figure 1.
Rice. 1.
Arteries and veins/venous plexuses at the base of the brain [11]. 1 - sphenoid-parietal venous sinus, 2 - middle cerebral artery (MCA), 3 - middle cerebral vein (deep), 4 - posterior cerebral artery (segment P1) (PCA), 5 - basilar venous plexus, 6 - basilar (main ) artery, 7 - vein of Rosenthal (right) and branch of the posterior cerebral artery (right), 8 - vertebral artery (segment V1), 9 - marginal venous sinus, 10 - vein of Galen (great cerebral vein), 11 - straight sinus, 12 - branch of the posterior cerebral artery (left), 13 - vein of Rosenthal (left), 14 - inferior ventricular vein.
Variants of normal and pathological venous blood flow are shown in Table 2 and Figures 2-18.
table 2
. Variants of normal and impaired venous blood flow in C- and PW-regimes. Causes of venous discirculation in the main venous pools. *
| Blood Flow Options | Causes of venous discirculation |
| Rosenthal's Vienna Fig. 2, 3, 4 |
|
| Inferior ventricular vein (tributary vein of Rosenthal) Fig. 5 | |
| Middle cerebral vein Fig. 6, 7, 8 |
|
| Vienna Galena Fig. 9, 10, 11 |
|
| Vertebral vein Fig. 12, 13 |
|
| Internal jugular vein Fig. 14, 15 |
|
| External jugular vein Fig. 16 | |
| Sphenoparietal venous sinus Fig. 17, 18 |
Note
*
The following should also be considered as possible causes of venous discirculation:
- violation of the central regulatory mechanisms of vascular tone;
- hereditary constitutional predisposition, manifested by undifferentiated connective tissue dysplasia (including in the form of bone deformities and hypermobility of the joints of the cervical spine);
- consequences of perinatal pathology (cervical spine injuries [12]; perinatal hypoxic-ischemic processes [13]);
- extravasal causes of venous stagnation: tumors of the mediastinum and neck; osteochondrosis of the cervical spine; traumatic compression of the chest and abdomen, leading to compression of the superior vena cava, jugular and vertebral veins; early osteochondrosis; deforming arthrosis; spondylosis; craniovertebral anomalies (basilar compression; defects of the odontoid process of the second cervical vertebra, Kimmerle anomalies; Arnold-Chiari anomalies);
- disorders of exclusively myogenic nature; compression of the vertebral artery by the inferior oblique muscle of the capitis during tonic tension with subsequent contracture or compression by the anterior scalene muscle;
- vasculitis of cerebral vessels, rheumovasculitis, bacterial meningitis, thrombosis of intracranial venous sinuses [10].
**
The literature covers various methods for invasive and non-invasive assessment of intracranial pressure (ICP) [7, 14]. In the specialized literature, the possibility of assessing ICP by displacement of the tympanic membrane is discussed [15]. However, this technique is described only for patients with hydrocephalus. The development of non-invasive methods for measuring ICP is still relevant, with various ultrasound and telemetric measurement methods taking the leading place. However, the question of the accuracy of the data obtained with non-invasive methods remains open and requires further clarification. None of the non-invasive techniques allows you to measure the absolute value of ICP, but only extrapolates its dynamics.
The only possible method for identifying ICH in patients with chronic venous insufficiency remains a comprehensive clinical and instrumental diagnosis, including assessment of the neurological status, condition of the fundus, Echo-encephalography (EchoEG), Dopplerography of the vessels of the neck (USDG BCS) and brain (TG USDG). Only the combination of these methods can bring the researcher closer to the expected conclusion. According to H. Bode [16], it is almost impossible to detect an increase in ICP in a child with hydrocephalus, based only on Doppler data.
In the studies of Yu.A. Rosin [17] proved the presence of a pressure gradient between the vein of Galen and the straight sinus. During transoccipital examination in the oral part of the straight sinus, in the area where the vein of Galen flows into the straight sinus, high venous outflow (more than 50 cm/s) is detected in children, which significantly exceeds the blood flow in the veins of Rosenthal, internal cerebral veins and the inferior sagittal sinus.
At the same time, a number of authors note that an increase in the tone of the main cerebral arteries should be considered as a compensatory mechanism for facilitating venous outflow [18].
The main hemodynamic signs of benign intracranial hypertension with transcranial Dopplerography (TCD) are considered to be an increase in maximum velocity and increased pseudopulsation of blood flow in the cerebral veins and sinuses (veins of Rosenthal > 15 cm/s, vein of Galen > 20 cm/s and straight sinus > 30 cm/s )
[1]. It is assumed that during chronically ongoing processes in the cranial cavity, venous circulation suffers more significantly.
It has been noted that a sharp increase in the venous signal and a change in the physiological direction of blood flow along the internal ophthalmic vein to retrograde are detected on the side of the “focus” of brain damage in cases of cerebrovascular accidents and traumatic brain injury, accompanied by an increase in intracranial pressure [13].
Rice. 2.
Middle cerebral artery (MCA). Transtemporal access. Color Doppler mapping mode at the level of the anterior cerebral artery (ACA) (3), MCA (5), first (7) and second (8) segments of the PCA, vein of Rosenthal (9), vein of Galen (10), middle cerebral vein (4), inferior ventricular vein (tributary vein of Rosenthal) (6). Brain peduncles (pedunculi cerebri) (1; 2).
Rice. 3.
Middle cerebral vein (deep). Right there. Color flow control, PW mode. Flow scanning in the vein of Rosenthal. Vmax 15.88 cm/s.
Rice. 4.
Posterior cerebral artery (segment P1) (PCA). Transtemporal access. Color flow control, PW mode. Scanning of pathological accelerated flow in the vein of Rosenthal. Vmax 28.59 cm/s.
Rice. 5.
Basilar venous plexus. Transtemporal access. Color flow control, PW mode. MCA (1), PCA segment P1 (4), cerebral peduncles (6; 7), middle cerebral vein (2), vein of Rosenthal (5). Flow scanning in the inferior ventricular vein (inflow of the vein of Rosenthal) (3).
Rice. 6.
Basilar (main) artery. Transtemporal access. Color flow mode at the level of the ACA (1), MCA (2), first segment of the PCA (4), middle cerebral vein (3). Brain peduncles (pedunculi cerebri) (5; 6).
Rice. 7.
Vein of Rosenthal (right) and branch of the posterior cerebral artery (right). Right there. Color flow control, PW mode. Flow scanning in the middle cerebral vein (proximal segment).
Rice. 8.
Vertebral artery (segment V1). Transtemporal access. Color flow control, PW mode. Scanning of pathological accelerated flow in the middle cerebral vein (proximal segment). Vmax 24.62 cm/s
Rice. 9.
Marginal venous sinus. Transtemporal access. Color circulation mode at the level of the first segment of the PCA (3), vein of Rosenthal (4), vein of Galen (5). Brain peduncles (pedunculi cerebri) (1; 2).
Rice. 10.
Vein of Galena (great vein of the brain). Right there. Color flow control, PW mode. Flow scanning in the vein of Gallen. Vmax 21.18 cm/s
Rice. eleven.
Direct sine. Transtemporal access. Color flow control, PW mode. Scanning of pathological accelerated flow in the vein of Galen. Vmax 50 cm/s
Rice. 12.
Branch of the posterior cerebral artery (left). Longitudinal scanning in the projection of the V2 segment of the vertebral artery (1) and vertebral vein (2). Color flow control and PW mode. Vmax in the vertebral vein is 34.69 cm/s.
Rice. 13.
Vienna of Rosenthal (left). Longitudinal scanning in the projection of the V1 segment of the vertebral artery (1). Color flow control and PW mode. Pathological accelerated flow in the vertebral vein (2). Vmax 83.73 cm/s.
Rice. 14.
Inferior ventricular vein. Transverse scanning in the projection of the internal carotid artery (3), external carotid artery (2) and internal jugular vein (1). Color flow control and PW mode. Vmax in the internal jugular vein is 41.49 cm/s.
Rice. 15.
Transverse scanning in the projection of the internal carotid artery (1) and the tortuous internal jugular vein (2). Color flow control and PW mode. Pathologically accelerated turbulent flow in the internal jugular vein up to 80 cm/s.
Rice. 16.
Transverse scanning in the projection of the internal (1) and external (2) carotid arteries, external jugular vein (3). Color flow control and PW mode. Vmax in the external jugular vein is 22.88 cm/s.
Rice. 17.
Transtemporal access. Mode of color circulation at the level of the MCA (2), and the sphenoparietal venous sinus (1). Brain peduncles (pedunculi cerebri) (3).
Rice. 18.
Ibid (Fig. 17). Color flow control, PW mode. Flow scanning in the sphenoparietal venous sinus (1). Vmax 19.19 cm/s.
Another problem facing the researcher, even in the case when it is possible to assess the nature of venous blood flow at the intra- and extracranial level, is the correct interpretation of the results obtained. Since the available literature data does not provide a holistic picture of the causes of venous discirculation, and in some cases, increased ICP or connective tissue dysplasia is indicated as the main reason for its occurrence, without indicating the possible mechanisms of the formation of venous discirculation, the benefit of such conclusions is extremely small. It is also impossible to influence the tactics of further treatment, since the points of possible application of efforts by doctors of different specialties are unknown or not indicated.
An increase in ICP as a probable cause of venous discirculation should not be forgotten that due to its low prevalence in the population (0.025-0.05% among children and adolescents), this pathology cannot be considered as the leading etiological cause of dysgemia and is most likely a diagnosis of exclusion.
Functional disorders of the musculoskeletal system with the formation of blocks in small joints of the spine with the appearance of reflex musculoskeletal pain syndromes are unreasonably rarely diagnosed, and the role of myofascial pain syndromes, in which the muscle suffers primarily, is underestimated. An important role in this in children is played by certain injuries to the cervical spine in the anamnesis (mainly during childbirth). The literature describes the mosaic nature of emerging pathogenetic factors in the obstruction of the outflow of venous blood from the skull. At the same time, the leading place in the genesis of dynamic disorders of venous circulation belongs to myofascial pain syndrome of cervical localization. When myofascial pain syndrome is localized in the muscles of the craniovertebral junction, congestive venous disorders are caused by general algic processes in this zone, including functional blockades of the junction, while tunnel-compression mechanisms in this zone do not play a decisive role in venous discirculation. Tunnel-compression mechanisms of obstruction of venous blood flow are most relevant in the middle and lower cervical localization of myofascial pain.
Conclusion
Taking into account our data on the strong correlation between accelerated venous blood flow and tortuosity of the ICA, VA (as indirect manifestations of disorders in the cervical spine, including manifestations of natal trauma to the cervical spine), we believe that in children and adolescents a key role in The appearance of dysgemia (impaired venous outflow) is played by the “pathology/structural features” of the cervical spine and the congenital structural features of the ICA at the extracranial level. The main causes of dysgemia in childhood should be considered “congenital connective tissue dysplasia” [19], manifested in the form of pathology of the cervical spine, with curvature and tortuosity of the bone canal, or “birth injuries with subluxation of 1-2 cervical vertebrae” (presence of a history of in the majority of examined individuals), with impaired venous outflow at the extracranial level.
Taking into account all of the above, it should also be concluded that if a picture of venous discirculation is identified, especially in young people, treatment should be aimed primarily at restoring the functional integrity of the musculoskeletal system of the cervical spine, correcting posture, manual practices, as well as compliance with regime-restrictive measures [20].
Literature
- Lelyuk V.G., Lelyuk S.E. Ultrasound angiology. M.: Real Time, 2003. 322 p.
- Valdueza JM, Schmierer K., Mehraein S., Einhäupl KM Assessment of normal flow velocity in basal cerebral veins. A transcranial Doppler ultrasound study. 1996. Stroke 27. pp. 1221-1225.
- Schoser BG, Riemenschneider N., Hansen HC The impact of raised intracranial pressure on cerebral venous hemodynamics: a prospective venous transcranial Doppler ultrasonography study // J. Neurosurg. 1999. V. 91, N 5. P. 744-749.
- Stolz E., Jauss M., Horning C. Cerebral venous anatomy in color-coded duplex sonography. What is possible in non-contrast enhanced TCCD? // New trends in cerebral haemodynamics and neurosonology / Eds. Kligelhofer J., Bartels E., Riglenshtein B. 1997. P. 312-319.
- Baumgartner RW, Gonner F., Muri R. Normal haemodynamics in cerebral veins and sinuses: a transcranial color-coded duplex sonography study // New trends in cerebral haemodynamics and neurosonology / Eds. Kligelhofer J., Bartels E., Riglenshtein B. 1997. P. 312-319.
- Aaslid R. Cerebral hemodynamics // Transcranial Doppler / Eds. Newell DW, Aaslid R.: - NY: Raven, 1992. R. 500.
- Shakhnovich V.A. Violation of the venous circulation of the brain according to transcranial Dopplerography // Ultrasound Doppler diagnostics of vascular diseases / Ed. ed. Nikitina Yu.M., Trukhanova A.I. M.: Vidar, 1998. pp. 355-400.
- Dicheskul M.L., Kulikov V.P., Maslova I.V. Ultrasound characteristics of venous outflow through the vertebral veins / Ultrasound and functional diagnostics, 2008, N 4. P. 33-40.
- Ivanichev G.A., Dolgikh G.B. Disturbances of arterial and venous blood flow in children with vertebrobasilar insufficiency // Journal of Neurology and Psychiatry, 2007, N 3.
- Dolgikh G.B., Ivanichev G.A. Cerebral vascular disorders in children with cerebral palsy and convulsive syndrome // Kazan Medical Journal, 2008, N 3.
- Pucillo M.V., Vinokurov A.G., Belov A.I. Atlas “Neurosurgical Anatomy” / Ed. Konovalova A.N. M.: Antidor, 2002.
- Burtsev E.M., Andreev A.V., Dyakonova E.N., Kutin V.A. Functional Dopplerography in pediatric angioneurology // Abstracts of the report at the VIII International Conference: Current state of non-invasive diagnostic methods in medicine. Sochi, 2001. pp. 151-160.
- Nikitin Yu.M., Trukhanov A.I. Ultrasound Doppler diagnostics in the clinic. MIC, 2004. 496 p.
- Adelson PD, Bratton SL, Carney NA et al. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Pediatr. Crit. Care Med. 2003; (4) 3.
- Samuel M., Burge DM, Marchbanks RJ Tympanic membrane displacement testing in regular assessment of intracranial pressure in eight children with shunted hydrocephalus // J. Neurosurg. 1998. V. 88. R. 983-995.
- Bode H. Pediatric application of transcranial Doppler sonography / Wien; Ny: Springer Verlag, 1988. P. 108.
- Rosin Yu.A. Dopplerography of cerebral vessels in children / SPbMAPO, 2006. 114 p.
- Belkin A.A., Alasheev A.M., Inyushkin S.N. Transcranial Dopplerography in intensive care. Methodological manual for doctors. Ekaterinburg: Publication of the Clinical Institute of the Brain of the Scientific Research Center of the Russian Academy of Medical Sciences; 2004.
- Andreev A.V., Lobanova L.V., Ermolin I.E. Transcranial Dopplerography and variational pulsometry in the diagnosis of cerebral angiodystonia in children // Journal of Neuropathology and Psychiatry. 1994. N 3. S. 22-23.
- Tsokolov AV, Tsokolova VA, Tsokolova MA, Senchilo VG, Egorov AU Venous discirculation // Journal of the Neurological Sciences. 333 (2013). e518. Abstract - WCN 2013, No102, Topic:8 - Headache. Vienne, Austria. 2013. Neurology in the age of globalization. XXI World Congress of Neurology.
Ultrasound scanner HS60
Professional diagnostic tools.
Assessment of tissue elasticity, advanced 3D/4D/5D scanning capabilities, BI-RADS classifier, options for expert cardiological studies.
Self-massage in the collarbone area
Working out certain points improves blood flow through the jugular veins. This will help immediately reduce or completely eliminate headaches caused by blood stagnation. If you do this self-massage regularly, the veins will become more elastic, resilient and begin to work like pumps, draining blood from the head in time. Accordingly, headaches will stop without taking medications. This is important because any drugs have side effects, including those delayed over time. It is imperative to use the body’s natural ability to heal itself.
Self-massage technique step by step:
- Place two fingers in the middle of the collarbone - just above the jugular fossa.
- Lightly press on the point - the pressure should not be strong, but should feel pleasant.
- Start working the point with circular rotations clockwise or counterclockwise - whichever is more comfortable for you.
- Do 20-30 rotations.
- Move to the other side of the neck and repeat steps 1-4.
Important! Please note again that you cannot put pressure on the point. Throughout the self-massage there should be pleasant sensations, and after its completion - a feeling of vigor or pleasant relaxation (depending on the time of day). This is a marker that you are doing everything right.
How often to perform
Everything is individual here. For some, it will help the first time and the headache will subside for a long time, for others, several sessions in a row are needed, and then maintain the condition of the veins with preventive self-massage.
If you have a diagnosed migraine, you need to start working on the point as soon as the first signs of pain appear. As soon as there is the slightest hint of imminent pain, we immediately do it. This will certainly reduce the intensity of pain and will most likely stop its further development. That is, a terrible migraine attack, for which even pills don’t help, simply won’t happen, your head will hurt a little, but it will go away after working on the clavicular point.
To prevent migraines, if they happen several times a month or a year, it is useful to do self-massage every week. This will help maintain the elasticity of the veins and blood vessels, so the blood will circulate correctly, without stagnation. The risk of not only headaches, but also increased intracranial pressure will be reduced.
Symptoms of stagnation
To identify problems with the venous outflow of blood in the brain, you should pay attention to the following symptoms:
- headache worsens when a person tilts or turns his head;
- headache when worrying and drinking alcohol;
- veins in the fundus of the eye expand;
- causeless dizziness, frequent headache in the morning;
- noises in the head and pain in the ears;
- swelling of the lower eyelids, cyanosis (blueness) of the face;
- causeless fainting;
- numbness of the limbs, decreased sensitivity;
- venous blood pressure is 50–80 mmH2O. Art.;
- mental disorders;
- It’s hard to lie down and lower your head.
If the venous outflow is disrupted, other symptoms may appear: problems with metabolism arise, intracranial pressure increases. In order to maintain firmness and clarity of mind in old age, one should not forget to take care of the functioning of blood vessels and the brain as a whole and to notice symptoms in time and carry out the necessary treatment.
Working out the back of the neck
As we have already found out, the problem arises due to compression of blood vessels, which is a consequence of the incorrect position of the vertebrae. Gymnastics will help solve and even more so prevent such a situation. For urgent help, you can gently influence the vessels. Let's take a closer look at how to do all this.
Gymnastics for the neck
Gymnastics should be performed regularly. Spend just 3-5 minutes a day and you will almost 100% protect yourself from headaches. A bonus is the prevention of high blood pressure – both intracranial and arterial.
There are many sets of exercises for the neck; you can see in detail, with step-by-step instructions and explanations, in Dr. Shishonin’s publications on cervical osteochondrosis. You've probably already read these articles and watched the videos, so let's briefly remind you. Tilts and rotations of the head, movements of the neck should not be performed abruptly, but carefully, so that there are pleasant sensations similar to those you experience when stretching after sleep.
Triggering a reflex response
The back of the neck can be treated with a piece of ice. The temperature effect causes a reflex reaction of the vessels: they react by restoring their shape. Dr. Shishonin spoke in detail about these techniques in specialized articles on cervical osteochondrosis.
Here we just remind you that you need to work with ice carefully. Don’t be afraid, you physically won’t be able to harm yourself, but don’t overdo it, otherwise the effect will be worse than from a delicate influence.
Vascular diseases of the brain. It can all start with a headache
Lev Manvelov, Candidate of Medical Sciences
, Albert Kadykov,
Doctor of Medical Sciences
“Science and Life” No. 2, 2007
General diagram of the blood supply to the brain.
Blood enters the brain through four large main arteries: two internal carotid and two vertebral. At the base of the brain stem, the vertebral arteries merge into one, the basilar artery. In the brain, the internal carotid artery divides into two main branches: the anterior cerebral artery, which supplies blood to the anterior parts of the frontal lobes, and the middle cerebral artery, which supplies parts of the frontal, temporal and parietal lobes. The vertebral and basilar arteries supply blood to the brain stem and cerebellum, and the posterior cerebral arteries supply the occipital lobes of the brain (image: Science and Life)
Headache, noise and dizziness, memory impairment, increased fatigue, decreased performance - such symptoms occur not only in the elderly, but also in middle-aged and even young people. Often, patients and some medical professionals do not take such complaints very seriously. Meanwhile, they may indicate chronic cerebral circulatory failure.
Blood supply to the brain
The normal functioning of the brain requires a large amount of energy. Nutrients and oxygen are delivered to the cells of the nervous tissue through the bloodstream. Nature has taken care to create a high degree of reliability of blood supply to the brain. It is provided by four powerful main arteries: two carotid and two vertebral. At the base of the brain, the branches of these vessels form a closed circle, called Willisian after the English physician and anatomist of the 17th century, Thomas Willis, who first described it. Thanks to this, the lack of blood supply in one of the main vessels is compensated by others. It also happens that even with serious disturbances in blood flow in three of the four main vessels, a person complains only of a slight deterioration in well-being - the compensatory capabilities of the brain are so great. Great, but, unfortunately, not unlimited. Man manages to “shatter” these perfect compensation mechanisms created by nature. It all starts with the most ordinary complaints of headache, dizziness, memory loss and fatigue.
After some time, the patient develops more serious neurological symptoms, indicating multiple brain damage. The reason for this is chronic cerebral circulatory failure, or “dyscirculatory encephalopathy.” This term was proposed in 1971 by famous domestic scientists working at the Research Institute of Neurology of the Russian Academy of Medical Sciences, Academician of the Russian Academy of Medical Sciences E.V. Schmidt and Candidate of Medical Sciences G.A. Maksudov, and it means changes in the brain associated with disturbances in its blood supply.
The main causes of the occurrence and development of dyscirculatory encephalopathy are arterial hypertension and atherosclerosis.
More than 40% of the adult population of Russia suffers from hypertension. Men and women, old people and young people get sick. Only in 5% of cases the cause of hypertension is clear. These may be renal failure, endocrine disorders, atherosclerosis and some other diseases. In 95% of cases, the cause of hypertension remains unclear, which is why it is called essential (literally, hypertension itself). With hypertension, the walls of blood vessels become denser, local narrowings (stenoses) and tortuosity are formed. All this leads to circulatory disorders, including blood supply to the brain. Sometimes it comes to occlusion - complete closure of the lumen of the vessel.
Blood clots, thrombi, develop in the area of atherosclerotic plaques that form on the inner walls of the vessel. Blood clots can completely block even large vessels, causing serious cerebrovascular accidents. (Image: Science and Life)
Unlike hypertension, the cause of atherosclerosis is known - it is a disorder of lipid metabolism. In patients with atherosclerosis, the level of fat-like substances in the blood increases - cholesterol, low-density lipoproteins, triglycerides, which are deposited on the walls of blood vessels, forming lipid stains. Then the spots grow into so-called plaques. Due to the deposition of calcium salts, the plaques become denser and ultimately narrow or even close the lumen of the blood vessels. Then they begin to disintegrate, their particles - emboli - enter the bloodstream and sometimes clog other small and large vessels.
Sometimes the development of dyscirculatory encephalopathy is facilitated by osteochondrosis, since in this disease, due to deformation of the intervertebral discs, the vertebral arteries that supply the brain with blood can be pinched.
Impaired blood supply leads to the gradual death of neurons in various parts of the brain, and the patient experiences neurological symptoms. Discirculatory encephalopathy is most characterized by emotional and personal disturbances. At the onset of the disease, asthenic conditions are noted: general weakness, irritability, poor sleep. Asthenia is often accompanied by depression. Gradually, such painful personality traits as egocentrism and periodically occurring causeless agitation begin to appear, which can be pronounced and manifest itself in inappropriate behavior. With further development of the disease, emotional reactivity decreases and gradually turns into dullness and apathy.
Once it begins, the disease steadily progresses, although during its course both sharp periodic deterioration (paroxysmal course) and periods of slow increase in symptoms of the disease can be observed.
We should not forget that dyscirculatory encephalopathy increases the risk of many severe brain diseases and, above all, stroke - an acute circulatory disorder of the brain (Manvelov A., Candidate of Medical Sciences; Kadykov A., Doctor of Medical Sciences. “Stroke is a social problem and medical” // “Science and Life” 2002, No. 5.). In Russia, strokes are registered in more than 400 thousand people per year. Of these, 35% die in the first three weeks of the disease, and only half of the patients reach the annual milestone. The possibility of epileptic seizures occurring against the background of developing discirculatory encephalopathy should not be excluded.
Types of chronic insufficiency of blood supply to the brain
Brain with blood vessels ( bottom view
).
The branches of the main vessels of the brain at its base form a vicious circle called the circle of Willis.
Thanks to this, if one of the vessels is narrowed or blocked, the blood supply to the brain is fully or partially restored. (Image: Science and Life) There are three main types of cerebrovascular accidents.
In Binswanger's disease, due to thickening of the walls and narrowing of the lumen of small arteries, diffuse damage to the internal structures of the brain occurs - the so-called white matter. Multiple small lesions are areas of dead neurons. In patients, circadian (daily) pressure fluctuations are disrupted: at night it either drops too sharply, or, conversely, increases, although the pressure should decrease slightly at night. One of the main symptoms of the disease is sleep disturbance. The patient has trouble falling asleep or sleeps with frequent awakenings. Other typical signs are the slow progression of memory and intelligence impairments up to dementia (dementia); increasing gait disturbances, urination and defecation disorders. It is known that Binswanger's disease can occur even at a relatively young age - up to 35 years.
Another type of dyscirculatory encephalopathy - the so-called multi-infarct conditions - is characterized by multiple small infarctions in the brain (micro-strokes). This means that in a certain area of the brain, due to blockage of the vessel, necrosis of the nervous tissue occurs. This affects both the superficial (gray matter) and deep (white matter) structures of the brain.
The main reason for the development of multi-infarction conditions is the narrowing and hardening of intracerebral arteries during arterial hypertension. Another common cause is heart disease accompanied by atrial fibrillation. In such patients, blood clots form in the cavities of the heart - thrombi, which can clog the vessels supplying the brain with blood. Increased blood clotting also contributes to the formation of blood clots. Another cause of multi-infarction conditions is atherosclerotic damage to intracerebral arteries.
Discirculatory ecephalopathy also develops with damage to the main (carotid and vertebral) arteries, which are not located inside the brain, but provide blood flow to the brain. Lesions can have different natures and causes - thrombosis, stenosis, bends and kinks of various etiologies.
There are three stages of dyscirculatory encephalopathy. The duration of each of them may be different. Much depends on the degree of hypertension or atherosclerosis, lifestyle, habits, heredity, concomitant diseases, etc. At the initial stage of the disease, people often complain of headaches, dizziness, noise in the head, decreased memory (non-professional) and performance. Patients are absent-minded, irritable, tearful, and their mood is often depressed. They usually have difficulty switching from one activity to another.
Functional areas of the brain.
When the blood supply to certain areas of the brain is disrupted, patients experience corresponding neurological symptoms (image: Science and Life)
At the next stage of the disease, memory impairment, including professional memory, progresses. The range of interests narrows, rigidity of thinking (obsession on some problem), incompatibility appear, the intellect suffers, and a change in personality occurs. Such patients are characterized by daytime sleepiness and poor night sleep. Neurological symptoms intensify, movements slow down, their coordination is impaired, mild speech disturbances appear, staggering when walking, and performance is significantly reduced.
At the last stage of the disease, gross changes in brain tissue make neurological symptoms even more pronounced, and mental disorders intensify, including dementia (dementia). Patients completely lose their ability to work, stop recognizing loved ones, perform inappropriate actions, and may get lost when going for a walk.
Diagnosis of encephalopathy
When examined, the vast majority of patients with discirculatory encephalopathy reveal characteristic diseases or physiological characteristics and habits. These risk factors include:
- arterial hypertension (blood pressure from 140/90 mm Hg and above);
- heart diseases (coronary disease, rheumatic lesions, heart rhythm disturbances, etc.);
- diabetes;
- excess body weight;
- sedentary lifestyle;
- hypercholesterolemia (total cholesterol above 6.2 mmol/l);
- long-term and frequent neuropsychic overstrain (stress);
- family history of cardiovascular diseases (stroke, myocardial infarction or arterial hypertension in close relatives);
- smoking;
- alcohol abuse.
Men with rapidly progressing dyscirculatory encephalopathy usually have a history of psycho-emotional stress, a sedentary lifestyle, alcohol abuse, lack of regular treatment and the presence of two or more concomitant diseases. In women, in addition to the listed factors, excess body weight often contributes to the unfavorable course of the disease.
If patients with arterial hypertension and atherosclerosis (or representatives of other risk groups) have complaints of headache, dizziness, decreased performance, memory impairment, then the initial stage of dyscirculatory encephalopathy can be suspected. Patients with such symptoms should, first of all, constantly monitor blood pressure, undergo an electrocardiographic examination, complete general blood and urine tests, and blood tests for sugar and lipids. A psychological study to assess the state of memory, intelligence, attention and speech would not hurt.
Even small nonspecific changes in the electrocardiogram can be harbingers of cardiovascular diseases, manifested in impaired blood circulation in the brain. By the way, normal electrocardiograms or echocardiograms do not exclude the presence of the disease, since changes can only be noticeable at the time of myocardial ischemia (anemia) or an attack of angina. An electrocardiogram taken during physical activity provides important information. Daily monitoring of heart function also allows you to identify abnormalities.
Information about the condition of the fundus (the back wall of the eye), the cells of which are directly connected to the neurons of the brain, is important for making a diagnosis. Changes in the blood vessels and nerve cells of the fundus make it possible to judge about disturbances in the structure of the brain tissue. In patients with discirculatory encephalopathy, hearing is often reduced, the swallowing reflex and sense of smell are impaired. Therefore, to make a diagnosis, it is necessary to conduct an otoneurological study that reveals disorders of the vestibular apparatus, auditory, olfactory and taste perceptions.
Useful information is provided by studying the rheological properties of blood - its fluidity. The main factor influencing the fluid properties of blood and the degree of its saturation with oxygen is considered to be hematocrit - the ratio of the volume of red blood cells to the volume of plasma. Its increase increases blood viscosity and worsens blood circulation. There is a direct connection between high hematocrit and cerebral infarctions.
After preliminary studies, the patient is usually referred for an X-ray examination of the cerebral vessels - angiography. Doctors consider angiography to be the “gold standard” with which the results of other research methods are compared. After the administration of a special contrast agent, X-ray images of the brain vessels are obtained. Angiography provides information about the duration and sequence of filling of blood vessels, about the formed “bypass” circulatory pathways in case of blockage or narrowing of cerebral vessels. The results of the study are important when deciding on the feasibility of surgery.
Electroencephalography is an old and very common method of studying the brain, based on recording its electrical potentials. Changes in the encephalogram indicate organic changes in the brain tissue, therefore, at the initial stage of the disease with dyscirculatory encephalopathy, encephalography may not reveal any abnormalities.
A real revolution in brain research was made by the advent of computed tomography, which combines the achievements of radiography and computer data processing methods. With its help, you can obtain not indirect, but direct data about brain structures and their changes. The method allows you to determine the location and size of brain lesions and their nature.
Magnetic resonance imaging of the brain.
Image of a healthy brain (A); changes in the brain matter in Binswanger's disease - rarefaction of the white matter of the brain (B); hydrocephalus - accumulation of fluid in the brain tissue - manifests itself in the form of expansion of the grooves and ventricles of the brain (shown by arrows) (B); multi-infarct condition - dead nerve tissue appears as small dark spots (shown by arrows) (D). Image: Science and Life
Recently, magnetic resonance methods have been used to diagnose cerebral circulatory disorders: nuclear magnetic resonance, magnetic resonance imaging and magnetic resonance angiography. Nuclear magnetic resonance provides information about the physicochemical properties of brain structures, making it possible to distinguish healthy tissues from altered ones. Magnetic resonance imaging allows you to obtain images of the brain, determine the location, size, shape and number of lesions, and study cerebral blood flow. Magnetic resonance angiography is a modification of magnetic resonance imaging. With its help, you can study the passage and “caliber” of extracranial and intracranial arteries and veins.
Currently, highly informative methods for obtaining three-dimensional images of brain structures have been created and are successfully used: single-photon emission computed tomography and positron emission tomography.
Duplex scanning of the internal carotid artery.
A formed small atherosclerotic plaque is visible, the lumen of the vessel is slightly narrowed (A); later stage of atherosclerosis - the lumen of the vessel of the internal carotid artery is partially blocked by a large plaque (B); occlusion - complete closure of the lumen of the vessel with a plaque (B); artery tortuosity (D) (Image: Science and Life)
Ultrasound methods are widely used to examine patients not only in hospitals, but also in outpatient settings: Dopplerography and echotomography, duplex scanning and transcranial Dopplerography. Doppler ultrasound is used to identify lesions of the carotid and vertebral arteries. It makes it possible to obtain information about the profile of blood flow in the vessels. With duplex scanning, color contrast of flows allows you to more clearly distinguish between moving (blood) and stationary (vascular walls) objects. The main vascular lesions detected by transcranial Doppler ultrasound are blockages, stenoses, spasms and aneurysms. The most complete information about the state of the vascular system of the brain can be obtained by comparing data from various ultrasound methods. Recently, a new method of ultrasound diagnostics has appeared - transcranial sonography with color Doppler coding. With its help, you can “see” the structures of the brain through the bones of the skull.
Treatment of dyscirculatory encephalopathy
Doctors have long been aware of the so-called law of halves, based on the results of large epidemiological studies. Its essence is that half of the patients do not know about their disease, and of those who know, half are not treated. Of those receiving treatment, half take medications irregularly, i.e., treatment is ineffective. Consequently, only about 12% of patients receive treatment. Such a depressing picture emerges because, as the French writer Francois de La Rochefoucauld said, “we lack the character to obediently follow the dictates of reason.”
Meanwhile, it is known that arterial hypertension and the dyscirculatory encephalopathy caused by it are quite treatable. Research programs to combat arterial hypertension conducted both in our country and abroad have shown that with their help it is possible to reduce the incidence of stroke by 45–50% in five years. If the program to combat hypertension worked on the scale of the entire healthcare system in Russia, then in five years it would be possible to save the lives of more than two million people dying from stroke. And this is not counting the loss of patients with other damage to the brain, heart, kidneys, eyes and other organs caused by hypertension.
According to the recommendations of the World Health Organization and the International Society of Hypertension, its therapy should be based on two principles:
- To reduce the possibility of side effects, the antihypertensive drug is prescribed in minimal doses, and if the reduction in blood pressure is insufficient, the dose is increased.
- To achieve maximum effect, combinations of drugs are used (a low dose of another is added to a small dose of one).
Patients with discirculatory encephalopathy against the background of severe hypertension should not strive to reduce blood pressure to normal (below 140/90 mm Hg), as this can lead to a deterioration in blood supply to the brain; it is enough to reduce it by 10–15% from the initial level.
In addition to drug treatment, patients with hypertension must follow simple rules: limit the consumption of table salt (up to 5 grams per day - 0.5 teaspoon); take antiplatelet agents (medicines that prevent the formation of blood clots) for a long time, almost for life; take vitamins and vitamin complexes containing ascorbic acid (vitamin C), pyridoxine (vitamin B6) and nicotinic acid (vitamin PP).
For dyscirculatory encephalopathy caused by atherosclerosis, treatment has its own characteristics and involves a low-calorie diet (up to 2600–2700 kcal per day) with a limitation of animal fats. In case of persistent levels of total blood cholesterol (above 6.2 mmol/l), which persist for at least six months against the background of a strict diet, cholesterol-lowering drugs (statins) are prescribed.
To prevent the progression of multi-infarction states of the brain, combined antiplatelet and anticoagulant therapy is used. Anticoagulants (drugs that reduce blood clotting) are selected in accordance with blood clotting and prothrombin levels and are recommended to be taken almost for life. In this case, it is necessary to monitor the blood prothrombin level once every two weeks. Patients taking anticoagulants should report any signs of bleeding to their doctor.
In addition to treatment aimed at eliminating the causes of dyscirculatory encephalopathy, patients are prescribed symptomatic therapy aimed at reducing the severity of symptoms. To prevent memory loss and decline in intelligence, drugs that improve metabolism in the brain are used. For movement disorders, therapeutic exercises, massage and other methods of rehabilitation therapy are recommended. For dizziness, vascular drugs and agents that affect the autonomic nervous system are prescribed.
Often discirculatory encephalopathy manifests itself in the form of asthenic-depressive syndrome. For its symptoms, doctors prescribe psychotherapy, psychological assistance, and drug therapy: antidepressants, sedatives. But first of all, you should take care of creating a friendly environment in the family and at work. After all, another outstanding physician of the Middle Ages, Fr. Paracelsus.
In patients with severe narrowing of the great vessels of the head (over 70%), the issue of surgical intervention is decided. It refers to three types of operations: stenting (expansion of the lumen of a vessel using a special frame - a stent), reconstruction of the vascular system (connecting various vessels to each other, forming branches) or removing part of the vessel and replacing it with a prosthesis.
For the prevention of dyscirculatory encephalopathy, a healthy lifestyle is of no small importance: adherence to a work regime, a diet with limited salt, liquids (up to 1–1.2 liters per day), foods containing animal fats (fatty meats, liver, sour cream, butter , eggs, etc.), and high-calorie foods. In addition to fats, high-calorie foods include alcohol and confectionery. It is good that vegetables and fruits predominate in the diet. You should eat at least four times a day, distributing food according to calorie content as follows: breakfast before work - 30%, second breakfast - 20%, lunch - 40%, dinner - 10%. It is recommended to have dinner no later than two hours before bedtime. The interval between dinner and breakfast should not exceed ten hours.
Patients need to monitor their weight, but it should be reduced gradually. For a person leading a sedentary lifestyle, energy consumption averages 2000–2500 kcal per day. If a woman reduces the calorie content of food to 1200–1500 kcal, and a man to 1500–1800 kcal, then in a week they will lose 0.5–1 kg. This rate of weight loss is considered optimal. An increase in physical activity has a good preventive effect. Training increases the resistance of the cardiovascular system to physical activity, which is reflected in a decrease in heart rate and blood pressure. As a result, mood improves, self-confidence appears, depression, fears, headaches, dizziness, and sleep disturbances decrease or disappear altogether. Patients become physically stronger and more resilient. A significant improvement in the condition is observed when exercising 3-4 times a week for 30-45 minutes. However, even after short training sessions (15–20 minutes), the patient feels better.
Therapeutic exercise should be carried out regularly, with a gradual increase in load. The intensity of exercise is calculated using the maximum heart rate (the patient's age in years is subtracted from 220). For patients who lead a sedentary lifestyle and do not suffer from coronary heart disease, choose the intensity of physical exercise at which the heart rate is 60-75% of the maximum. Of course, before you start doing physical therapy, you should definitely consult with your doctor.
For patients at stages I and II of discirculatory encephalopathy, sanatorium-resort treatment is indicated. It is better if it is a cardiovascular-type sanatorium in a familiar climate.
Timely diagnosed discirculatory encephalopathy and properly selected complex treatment prolong an active, fulfilling life.
The authors express their gratitude to the staff of the State Research Institute of Neurology of the Russian Academy of Medical Sciences R.N. Konovalov, M.A. Kravchenko, A.V. Kadykov for help in illustrating the article.