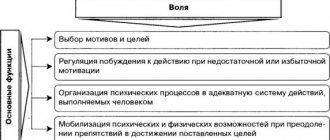
Emotional - volitional disorders in children and adolescents, psychological support
author: Bekhtereva Natalya Vladimirovna
Teacher - psychologist State government educational institution of the Sverdlovsk region "Novouralsk school No. 2, implementing adapted basic general education programs"
Emotional - volitional disorders in children and adolescents, psychological support
EMOTIONAL-VOLITIONAL VIOLATIONS
IN CHILDREN AND ADOLESCENTS,
PSYCHOLOGICAL SUPPORT
Bekhtereva Natalya Vladimirovna
teacher - psychologist
State government educational institution of the Sverdlovsk region “Novouralsk School No. 2, implementing adapted basic general education programs”
Nowadays, it is increasingly possible to meet families in which children not only do not want to study, but generally do not attend school for several months. The urgency of the problem affects not only one family, but also society as a whole.
«
Motivation is a psychophysiological process that, under the influence of external or internal factors, stimulates people’s desire to engage in a particular activity.”
Motivation can be internal and external.
We can talk about internal motivation when a person does something simply for pleasure, interest, or achieving a goal.
With external motivation, activity is aimed at achieving certain goals. Moreover, they may not be directly related to the nature of this activity - for example, a child may go to school not because he wants to study, but so as not to be scolded by his parents (coercion and threat of punishment), for rewards, or to communicate with friends. External motivation is the stimuli that come to us from other people or circumstances. As for children, their external motivation is often coercion from an adult. That is, a child starts studying only because he was forced, intimidated, and not at all because he was instilled with an interest in learning new things. The development of the emotional volitional sphere proceeds in parallel with the formation of the child’s motivation and needs, and is one of the most important conditions for the development of the child’s personality. The development of the emotional sphere is facilitated by family, school, and all the life that surrounds and constantly influences the child. The emotional-volitional sphere is recognized as the primary form of mental life, the “central link” in the mental development of the individual.
In the process of growing up, a child faces problems that he has to solve with varying degrees of independence. Attitude to a problem or situation causes a certain emotional response, and attempts to influence the problem cause additional emotions. For the correct emotional-volitional development of a child, increasing ability to control the expression of emotions is essential.
The main causes of violations are:
- suffered stress;
- retardation in intellectual development;
- lack of emotional contacts with close adults;
- social and everyday reasons (asocial families);
- films and computer games not intended for his age;
- a number of other reasons that cause internal discomfort and feelings of inferiority in the child.
Violations in the emotional-volitional sphere of a child’s personality have characteristic features of age-related manifestations.
In preschool age, excessive aggressiveness or passivity, tearfulness, “getting stuck” on a certain emotion, inability to follow norms and rules of behavior, and insufficient development of independence are observed.
At school age, these deviations, along with those listed, can be combined with self-doubt, impaired social interaction, decreased sense of purpose, and inadequate self-esteem.
The main external manifestations are as follows:
- Emotional tension. With increased emotional tension, difficulties in organizing mental activity and a decrease in play activity characteristic of a particular age may be expressed.
- The rapid mental fatigue of a child in comparison with peers or with earlier behavior is expressed in the fact that the child has difficulty concentrating, he may demonstrate a clear negative attitude towards situations where the manifestation of thinking and intellectual qualities is necessary.
- Increased anxiety can be expressed in avoidance of social contacts and decreased desire to communicate.
- Aggressiveness. Manifestations can be in the form of demonstrative disobedience to adults, physical aggression and verbal aggression. Also, his aggression can be directed at himself, he can hurt himself. The child becomes disobedient and with great difficulty succumbs to the educational influences of adults.
- Lack of empathy. In case of disturbances in the emotional-volitional sphere, it is usually accompanied by increased anxiety. An inability to empathize may also be a warning sign of a mental disorder or intellectual disability.
- Unpreparedness and unwillingness to overcome difficulties. The child is lethargic and does not enjoy contact with adults. Extreme manifestations of behavior may look like complete ignorance of parents or other adults - in certain situations, a child may pretend that he does not hear an adult.
- Low motivation to succeed. A characteristic sign of low motivation for success is the desire to avoid hypothetical failures, so the child takes on new tasks with displeasure and tries to avoid situations where there is even the slightest doubt about the result. It is very difficult to persuade him to try to do anything. A common answer in this situation is: “it won’t work,” “I don’t know how.” Parents may mistakenly interpret this as a manifestation of laziness.
- Expressed distrust of others. It can manifest itself as hostility, often accompanied by tearfulness; school-age children can manifest it as excessive criticism of the statements and actions of both peers and surrounding adults.
- Excessive impulsiveness of a child, as a rule, is expressed in poor self-control and insufficient awareness of his actions.
- Avoiding close contacts with other people. A child may repel others with remarks expressing contempt or impatience, or impudence.
Currently, there is an increase in emotional and volitional disorders.
The lack of formation of the emotional-volitional sphere can manifest itself at different levels:
- Behavioral – in the form of infantile personality traits, negative self-presentation, impaired ability to manage one’s emotions and adequately express them;
- Social – in the form of violations of emotional contacts, a low level of formation of motives for establishing and maintaining positive relationships with adults and peers, maladjustment;
- Communicative – in the form of undeveloped skills to establish and maintain a constructive level of communication, to understand and adequately assess the state and feelings of the interlocutor in accordance with the situation;
- Intellectual - in the form of inability to distinguish and determine emotions and emotional states of people, difficulties in understanding the conventionality (non-obvious meaning) of a situation, difficulties in understanding relationships between people, a reduced level of development of higher emotions and intellectual feelings (feelings of beauty, the joy of knowledge and discovery, a sense of humor ), and in general in a decrease in social intelligence and competence.
There are two types of emotional and volitional disorders:
- Impulsive type. The child begins to commit unexpected and rash actions that cannot be called reasonable only because of the emotions he experiences. Reacts poorly to criticism; they show aggression to any comments. Characteristic of people suffering from psychopathy.
- Borderline type. It often manifests itself in adolescence; this disorder is expressed in the fact that a person overreacts to any life situations, begins to exaggerate his own failures, and has a hard time withstanding stress. Often the result of such instability is the use of drugs and alcohol, suicide and violations of the law.
Causes:
-Psychological trauma (chronic stress, prolonged emotional stress);
- Hyper or hypoprotection from loved ones (especially in adolescence);
— Psychasthenia;
— Hormonal imbalance (hormonal imbalance);
— Acute lack of nutrients (vitamins, minerals).
Emotional unformation (instability) can also accompany some somatic diseases (diabetes mellitus, vascular and organic diseases of the brain, traumatic brain injuries).
The most striking manifestations of emotional disorders are depressive and manic syndromes.
With depressive syndrome, three main signs can be observed in children and adolescents:
- Hypotomia (decreased mood).
The child is constantly yearning, feels depressed and sad,
shows reactions to joyful and other events.
- Associative inhibition (mental inhibition).
In its mild manifestations, it is expressed in the form of slowing down monosyllabic speech and taking a long time to think about the answer. A severe course is characterized by the inability to comprehend the questions asked and solve a number of simple logical problems.
- Motor retardation.
Motor retardation manifests itself in the form of stiffness and slowness of movements. In severe cases of depression, there is a risk of depressive stupor (a state of complete depression).
In manic syndrome, three main symptoms can be observed:
- Elevated mood due to hyperthymia (constant optimism, disregard for difficulties);
- Mental excitability in the form of accelerated thought processes and speech (tachypsia);
- Motor excitement.
Violations of the emotional and volitional sphere in children and adolescents must be treated comprehensively, taking into account psychological and physiological symptoms.
The school psychologist conducts a comprehensive psychodiagnostics of the student (methods and tests are used to assess the development and psychological state of the child, taking into account his age characteristics: art therapeutic techniques, Luscher color test, Beck anxiety scale, questionnaire “Well-being, activity, mood” (SAM), test Phillips school anxiety).
Correction of disharmonies in the development of a child’s personality, teach how to react correctly when stressful situations arise and control their feelings, teach children to cope with life’s difficulties, overcome barriers in communication, relieve psychological stress, create an opportunity for self-expression.
Consultative work with parents or persons replacing them, with the child.
A doctor is a neurologist (he will help treat neurological disorders, diagnose, prescribe drug therapy to form dynamic balance and a certain safety margin of the central nervous system).
Including other specialists of a narrow profile (endocrinologist, psychiatrist).
Comprehensive and timely treatment in children and adolescents helps to completely eliminate the symptoms of the disease. That is why the main role is given to parents.
Analyzing the experience of doctors, psychologists, and teachers, we can give the following recommendations for working with the emotional and volitional sphere in children and adolescents:
- Create a clear daily routine for your child. This helps stabilize his unbalanced nervous system.
- Keep a close eye on the stress in your child's life. At the first signs of neurological distress, a consultation with a neurologist is necessary.
- Adequate physical activity is necessary; it reduces mental stress (sports sections, “Sports – Hour”).
- If there are psychological problems in the family, consultation with a school psychologist is necessary.
- If possible, ensure that your child visits a child psychologist; various areas are used to correct emotional disturbances (art therapy, play therapy, fairy tale therapy, ethnofunctional psychotherapy, relaxation exercises).
Prevention of emotional states in children and adolescents in an educational institution is as follows:
— Knowledge of the family environment and the child’s predisposition to neurotic reactions.
— A benevolent atmosphere in the lesson, mitigating emotional discomfort (the teacher must constantly reinforce the child’s success, stimulate him to perform the activity with tips, approval, praise, and constant statements of success).
— Increasing activity and independence among students.
-Correction of self-esteem, level of consciousness, formation of emotional stability and self-regulation.
— Choosing the right communication style.
- Involvement in active creative forms of activity (meaningful assessment of its results, all kinds of emphasizing achievements and a number of other means should help improve the academic performance of children with neuroses).
— Increasing teacher self-control.
— Motor relief for children, physical education lessons.
Literature:
- Alyamovskaya V.G., Petrova S.N. Prevention of psycho-emotional stress in preschool children. M., Scriptorium, 2002.- 432 p.
- Benilova S. Yu. Special children - special communication // Journal of Education and training of children with developmental disorders, 2006. – No. 2.
- Bozhovich L.I. Personality and its formation in childhood. – St. Petersburg: Peter, 2008. – 400 p.
- Godovnikova L.V. Fundamentals of correctional and developmental work in mass schools: Textbook. allowance / Under scientific. ed. I. F. Isaeva. – Belgorod: BelSU Publishing House, 2005. – 201 p.
- Rozhenko A. Correction of the emotional-volitional sphere of the child // Social security, 2005 - No. 3 February - pp. 16-17.
- Semago N.Ya., Semago M.M. Problem children. Fundamentals of diagnostic and correctional work of a psychologist. M.: ARKTI, 2000.
Emotional - volitional disorders in children and adolescents, psychological support
syndromes of motor-volitional disorders
Category: Psychiatric Nursing/Clinical manifestations of major psychopathological syndromesSyndromes of motor-volitional disorders include catatonic syndrome. It manifests itself in two variants: catatonic agitation and catatonic stupor.
.
Catatonic arousal is expressed by stereotypical movements, their chaoticity, and pretentiousness. Along with this, unmotivated impulsive actions may unexpectedly arise. Patients suddenly jump up, run somewhere, attack others, in some cases show excessive rage, aggressiveness, which is replaced after a short time by calmness
.
The catatonic syndrome is characterized by echo symptoms:
- echolalia
- stereotypical repetition of heard phrases; - echopraxia
- repetition of movements seen in others; - echomicia
is an involuntary repetition of the interlocutor’s facial expression.
Catatonic stupor
-
characterized by immobility and mutism (refusal to talk, silence)
. Sometimes it manifests itself in the form of waxy flexibility - the patient can be given any position in which he freezes for a long time.
Often with catatonic stupor the following is observed:
- symptoms of an air cushion
- if you remove the pillow from under the head of a patient lying on the bed, the head hangs in the air, and he remains there for a long time; - proboscis symptom
- lips extended forward; - hood symptom
- pulling a robe over the head with an open face;
Symptoms of active and passive negativism
Active negativism is expressed in the fact that patients do everything the opposite, contrary to the request.
With passive negativism, the patient simply does not comply with requests and demands. Negativism is often manifested by patients refusing to eat.
Stupor with numbness may also occur, manifested by muscle tension, especially the flexors. Because of this, the patient assumes a fetal position, in which he remains for a long time.
Catatonic syndrome can occur with clear consciousness ( lucid catatonia
) and with oneiric disorders of consciousness (
oneiric catatonia
).
In the first case, despite stupor, mutism, negativism, the patient is oriented in the surrounding reality, notices everything around and, upon emerging from the stupor, can tell everything about what he heard and saw. In the case of oneiric catatonia, catatonic agitation with foolishness, interrupted speech, and dream-like visions is observed
.
Catatonic syndrome is an important symptom of schizophrenia. It also occurs in involutional reactive and epileptic psychoses.
Syndromes of disorders of the volitional sphere include apathetic-abulic syndrome, which is characterized by the gradual development of apathy (indifference) and abulia (lack of will). Such patients are inactive, indifferent to the environment, and do not show interest in family, friends, or events happening around them. They have no plans for the future, no desire for cognitive activity, no care for relatives, family, or themselves. Reactions of anger, hunger, and sexual functions persist somewhat longer.
Apathetic-abulic syndrome - characteristic of the clinical picture of schizophrenia, traumatic illness, brain tumor
.
See clinical manifestations of the main psychopathological syndromes
Saenko I. A.
Sources:
- Nurse's Handbook for Care/N. I. Belova, B. A. Berenbein, D. A. Velikoretsky and others; Ed. N. R. Paleeva. - M.: Medicine, 1989.
- Bortnikova S. M., Zubakhina T. V. Nervous and mental illnesses. Series 'Medicine for you'. Rostov n/d: Phoenix, 2000.
- Kirpichenko A. A. Psychiatry: Textbook. for honey Inst. — 2nd ed., revised. and additional — Mn.: Vysh. school, 1989.