Interstitial cystitis in women
Interstitial cystitis is a chronic bladder disease characterized by frequent, urgent urination and pain, which significantly affects the quality of life of patients. A feature of interstitial cystitis is that the inflammatory process develops and occurs in the submucosal layer of the bladder wall. Interstitial cystitis
is the most common cause of chronic pelvic pain in women.
Symptoms of interstitial cystitis
- Intense and almost constant pain in the bladder with interstitial cystitis
- Frequent urination accompanied by an urgent urge with interstitial cystitis
- Pain and discomfort during sexual activity with interstitial cystitis
The intensity of pain with interstitial cystitis ranges from mild burning and discomfort to severe, unbearable pain in the bladder, lower abdomen, perineum, pelvis, vagina, sacrum and thighs. Pain with interstitial cystitis increases as the bladder fills, reaching its peak at the height of the urge to urinate and during the first minutes after it. Typically, periods of exacerbation of interstitial cystitis and remission are not seasonal and individual for each patient.
Before the patient learns about his true diagnosis - interstitial cystitis
and begins to receive treatment, he goes through a long journey, several years long, which consists of weekly or monthly fruitless visits to doctors in clinics and private medical institutions. Typically, these patients undergo a large number of unsuccessful courses of treatment for interstitial cystitis with antibiotics, which are prescribed despite normal urinalysis and urine culture. Compounding the situation is the widespread belief in the need for outpatient treatment using harsh chemicals such as silver nitrate instilled into the bladder. The incidence of interstitial cystitis in women is 10 times higher than in men.
For doctors
Interstitial cystitis: conservative treatment. Part 1. Previous article
The diagnosis of interstitial cystitis
(Painful Bladder Syndrome)
can be made based on symptoms such as chronic pelvic pain, pressure or discomfort associated with bladder filling, accompanied by pollakiuria and/or urinary urgency. Further diagnosis is based on cystoscopy with hydrobouge and the results of morphological examination.
Conservative therapy of interstitial cystitis is aimed primarily at the so-called non-ulcerative form of interstitial cystitis, which is characterized by the absence of Hunner's lesions during cystoscopy, the presence of glomerulations during cystoscopy with hydrobouge and characteristic morphological changes (increased number of macrophages, granulation tissue, inflammatory infiltrate).
I. Oral therapy
Analgesics
Since pain is the main symptom of interstitial cystitis, reducing the intensity of pain is the primary goal of therapy. For this purpose, patients actively use non-steroidal anti-inflammatory drugs. Unfortunately, due to the involvement of the visceral and neuropathic components in the pathogenesis of pain in interstitial cystitis, NSAIDs are usually ineffective.
Narcotic analgesics are more effective and can be used for short-term pain relief when pain increases. Since interstitial cystitis is a chronic disease, long-term use of narcotic analgesics is possible in severe cases, but with extreme caution (1).
Glucocorticoids
Publications on the results of the use of glucocorticoids in interstitial cystitis are very contradictory and show both promising (2) and disappointing results (3). Soucy proposed the use of prednisolone in the ulcerative form of interstitial cystitis, refractory to other types of therapy (4). It should be noted that the serious side effects of glucocorticoids make their long-term use difficult.
Antihistamines
Macrophages are known to play an important role in the pathogenesis of interstitial cystitis. Since their degranulation releases many biologically active substances, including histamine, the use of histamine receptor blockers seems quite logical. There are studies on the results of using H1 (5) and H2 (6) receptor blockers, with rather contradictory results.
Hydroxyzine
Hydroxyzine (Atarax) is an H1 receptor blocker with interesting additional properties: it blocks neuronal activation of macrophages by inhibiting serotonin synthesis by thalamic macrophages. Side effects include drowsiness and general weakness, which, however, in most cases disappear during treatment (7). According to Theoharides, 90% of patients reported feeling better.
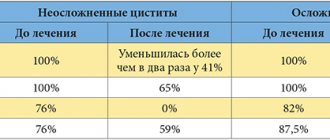
An interesting fact is that patients with interstitial cystitis and concomitant irritable bowel syndrome and migraine also showed a decrease in the symptoms of these diseases (5). In contrast to the impressive results of pilot studies (5,8), a prospective, randomized, placebo-controlled trial did not show a statistically significant difference between hydroxyzine and placebo (9). However, the combination of hydroxyzine and oral pentosan polysulfate was effective in 40% of cases, versus 13% with placebo.
Amitriptyline
The tricyclic antidepressant amitriptyline reduces the severity of pain, pollakiuria and urgency in interstitial cystitis. A possible mechanism of action of amitrityline is blockade of m-cholinergic receptors in the bladder, inhibition of the reuptake of serotonin and norepinephrine, and blockade of H1 receptors. In addition, amitriptyline is an anxiolytic (10).
Several studies have demonstrated the effectiveness of oral amitriptyline in interstitial cystitis (11–13). In one prospective study, 4 months of amitriptyline resulted in a statistically significant reduction in pain and urgency, while functional bladder capacity and pollakiuria changed, but not significantly (14).
In subsequent studies, 64% of patients showed a positive result after 20 months of taking amitriptyline. 46% of study participants reported good or excellent response to amitriptyline (15,16). Amitriptyline showed a statistically significant improvement compared with placebo. Side effects included weight gain and drowsiness.
Pentosan polysulfate
Pentosan polysulfate (Elmiron) is believed to help restore defects in the protective glycosaminoglycan layer of the bladder. A significant improvement in the symptoms of interstitial cystitis (pain, pollakiuria, urgency) was recorded as a result of a course of oral glycosaminoglycan replacement therapy with pentosan polysulfate. No improvement in nocturia was noted. Pentosan polysulfate therapy has been shown to be more effective in patients with Hunner's lesions of the bladder compared with nonulcerative interstitial cystitis (19).
The standard therapeutic dose of 150-200 mg twice daily between meals has demonstrated insufficient absorption in the gastrointestinal tract and, consequently, low bioavailability of the drug. One study compared doses of 300, 600 and 900 mg, which demonstrated sufficient effectiveness, which, however, was not dose-dependent. The effectiveness of oral glycosaminoglycan replacement therapy with pentosan polysulfate depended more on the duration of the course. Half of the study participants showed positive results after 32 weeks of pentosan polysulfate therapy. No significant side effects were noted.
In patients with insufficient effectiveness of oral therapy for interstitial cystitis with pentosan polysulfate, the effectiveness of subcutaneous injections of heparin was demonstrated according to the following scheme: starting dosage - 5000 units 2-3 times a day for 12 days, then moving to a maintenance dose of 5000 units 1 time per day for 6 months (required period for urothelial restoration) (21).
Chondroitin sulfate, sodium hyaluronate
So far, only a small number of studies have focused on the effectiveness of oral glycosaminoglycan replacement therapy with chondroitin sulfate and sodium hyaluronate (“IALuril” soft gels, “Urolife”). However, data from pilot studies indicate a reduction in pain and pollakiuria in patients with defects in the glycosaminoglycan layer of the bladder (interstitial and radiation cystitis). The dosage was 200 – 400 mg of chondroitin sulfate three times a day for 3-6 months. (36).
Antibiotics
The role of antibacterial drugs in the treatment of interstitial cystitis appears to be very limited, although some studies have demonstrated a decrease in pain and urgency with antibacterial therapy (22).
Immunosuppressants
According to Oravisto, azathioprine therapy reduces pain and pollakiuria in patients with interstitial cystitis (23). Pilot studies of the effectiveness of cyclosporine A (24) and methotrexate (25) demonstrated a good analgesic effect with a minor effect on pollakiuria and urgency.
Relatively recent studies of the effectiveness of cyclosporine A have shown promising results with significant reductions in urinary frequency, increases in functional bladder capacity, and increases in urine output after 1 year of therapy. With continued therapy, the achieved effect was maintained during 5 years of observation, with most patients reporting no pain in the bladder area. However, when therapy was discontinued, a recurrence of interstitial cystitis symptoms was observed after several months (26, 27).
Further studies (27) showed that a 6-month course of cyclosporine A was more effective compared with the same course of pentosan polysulfate for all symptoms of interstitial cystitis (75% of participants receiving cyclosporine noted positive changes compared with 19% in the group pentosan polysulfate).
However, significant side effects in the cyclosporine group (pain in the gums, muscles, abdomen, hot flashes, cramps, etc.) led to the discontinuation of participation in the study by some patients. Careful monitoring of the patient with regular measurement of blood pressure and assessment of blood creatinine levels is necessary during immunosuppressant therapy. The daily dose of cyclosporine A is 3-3.5 mg/kg body weight, twice a day.
Gabapentin
Gabapentin is a drug for the treatment of epilepsy, but is also widely used as a treatment for neuropathic pain. The use of gabapentin may reduce the dosage of other analgesics, including narcotics. In one study, two patients with interstitial cystitis reported increased functional bladder capacity and adequate pain relief after adding gabapentin to their treatment regimen (29).
In another study of 21 patients with chronic pelvic pain syndrome, 10 reported improvement after 6 months of gabapentin (30). The study involved 8 patients with interstitial cystitis, 5 of them reported a positive effect of gabapentin. The recommended starting dose of gabapentin is 300 mg 3 times a day, subsequently the daily dose is titrated to 1800 mg.
Pregabalin
Pregabalin (Lyrica) is one of two drugs approved by the FDA for the treatment of neuropathic pain (31) and is used to treat diabetic and postherpetic neuropathy. There are no studies on the effectiveness of pregabalin in interstitial cystitis, with the exception of a clinical case described by the Indian urologist Lakshmi.
A 52-year-old woman received 75 mg of pregabalin twice daily along with 10 mg of amitriptyline, noting a slight improvement. The starting dose of pregabalin is usually 75 mg twice daily, gradually increasing to 300 mg twice daily.
Quercetin
Quercetin is a bioflavonoid that may be effective for CPPS in men (33). Theoharides et al conducted a study on the effectiveness of CystoProtek (34), containing quercetin, chondroitin sulfate, and sodium hyaluronate. The patients' condition improved significantly after a 6-month course of therapy. Unfortunately, there are no data from comparative studies.
Tanezumab
Tanezumab is a human monoclonal antibody to nerve growth factor. Increased production of Nerve Growth Factor by macrophages is one of the reasons for the increase in the number of vanilloid and purine receptors in the urothelium and leads to the appearance of symptoms such as pain, urgency and pollakiuria. With the use of tanezumab, regression of these symptoms is observed after 6 weeks (35).
II. Instillations into the bladder
The advantage of intravesical administration of drugs is the creation of a high concentration of the active substance in the lesion with a minimum of side effects. The disadvantages are the need for catheterization, which can be painful in interstitial cystitis, and the risk of infectious complications.
Lidocaine
There are several publications on the successful treatment of interstitial cystitis using lidocaine instillation into the bladder (37,38). Alkalinization of lidocaine solution improves its pharmacokinetics (39). The CLParsons study showed that instillation of a combination of 1-2% lidocaine, heparin and sodium bicarbonate resulted in immediate relief of pain and irritative symptoms in 94% of patients (40). According to JCNickel, instillation of lidocaine and sodium bicarbonate for 5 days leads to improvement for up to 1 month (41).
Pentosan polysulfate
Pentosan polysulfate is also used intravesically, due to low bioavailability when taken orally. After 3 months of therapy with intravesical instillations of pentosan polysulfate, 40% of patients reported significant improvement, whereas in the group receiving placebo (saline) instillations, only 20% reported improvement (42). Bladder capacity increased only in the group receiving pentosan polysulfate.
After 18 months of therapy, 80% of the pentosan polysulfate group and 40% of the control group reported improvement. In another comparative randomized trial, women with interstitial cystitis were divided into two groups:
1) pentosan polysulfate orally and intravesical instillation;
2) pentosan polysulfate orally and intravesical instillation of placebo.
The course of instillations lasted 6 weeks, taking pentosan polysulfate per os lasted up to 12 weeks. Both groups showed improvement, but the improvement was greater in the combination therapy group (43).
Heparin
Instillation of heparin into the bladder has been proposed to protect the urothelium from the effects of potassium ions and also to restore its protective glycosaminoglycan layer. Half of patients with interstitial cystitis who received heparin instillation for 3 months reported improvement (44).
Kuo et al reported that 80% of participants with a positive KCl test reported improvement after 3 months of heparin instillation (45).
Baykal et al studied the effectiveness of heparin instillation in combination with electrical stimulation of the tibial nerve and noted a decrease in pain, pollakiuria and an increase in bladder capacity (46).
Hyaluronic acid (sodium hyaluronate)
Sodium hyaluronate is a natural proteoglycan that repairs defects in the glycosaminoglycan layer of the bladder. Positive results from sodium hyaluronate instillation were reported by 56% of patients at week 4 of therapy and by 71% at week 7 (47). After 24 weeks, the effectiveness of hyaluronic acid instillations decreased.
Nordling et al (48) and Kallestrup et al (49) published the results of a 3-year follow-up of patients who received sodium hyaluronate instillation for 3 months. A positive long-term effect was demonstrated by 2/3 of patients. Another study (50) showed similar results with hyaluronic acid instillations in patients with a positive KCl test.
Participants received weekly instillations of 40 mg sodium hyaluronate (50 ml 0.08% solution) for 10 weeks. Pain syndrome was assessed using a visual analogue scale. Also, one study assessed the long-term results of intravesical sodium hyaluronate (51). 50% of respondents reported complete remission without additional therapy and 41.7% reported improvement after a second course of treatment.
Chondroitin sulfate
Intravesical instillation of chondroitin sulfate (52) demonstrated efficacy in two non-randomized pilot studies. Steinhoff (53) instilled chondroitin sulfate once a week for 4 weeks and then once a month for 12 months.
Results after 3-12 weeks of therapy were as follows:
— good effect – 46.2%; — positive effect – 15.4%; — partial effect – 30.8%; – no effect – 7.7%.
In the second study (54), patients were treated with a high concentration of chondroitin sulfate solution (2%) - two instillations per week for 2 weeks and then a 0.2% solution once a week for 4 weeks, then once a month during a year.
Positive results were demonstrated by 73.1% of patients; the time to achieve maximum effect was 4-6 months. Maintenance instillations with a 2% solution were more effective than 0.2%. The results of comparative randomized placebo-controlled studies showed that the effectiveness of chondroitin sulfate instillations (39.4%) was higher than placebo (22.6%), although the difference was not statistically significant (55.56).
Dimethyl sulfoxide
The effectiveness of dimexide instillations for interstitial cystitis was found empirically, but is now standard treatment. In a placebo-controlled study, patients received instillations of dimexide once every two weeks - eight instillations per course. The therapy was subjectively effective in 53% of cases compared to 18% in the placebo group. Objective improvement was demonstrated by 93% versus 35%, respectively (57).
Despite the sufficient number of proposed treatment methods, interstitial cystitis still seems to be a practically incurable disease. Thus, the goal of therapy is to achieve a more or less long-term remission, or adequate control of pain and pollakiuria. For this purpose, the following are most often used:
Oral therapy:
- Amitriptyline - starting with 12.5 mg twice a day and increasing, if necessary, the dosage up to 100 mg/day;
— Atarax – 25 mg 2-3 times a day;
— Pentosan polysulfate – at least 900 mg/day in three doses with a course of treatment of at least 6 months;
— Chondroitin sulfate – at least 900 mg/day in three doses, 6 months
Intravesical therapy:
— Lidocaine 1-2% solution – instillation into the bladder 3–7 times a week
— Glucocorticoids
— Dimexide 5% — instillations into the bladder 2-3 times a week, 8 instillations per course of treatment;
- Sodium hyaluronate 0.08% or 0.12% solution - instillation into the bladder 1-2 times a week, up to 24 instillations per course of treatment;
-Heparin – 10,000 units intravesically, 1-2 times a week;
— Chondroitin sulfate 0.2%, 2% solution — instillations into the bladder 1-2 times a week, up to 24 instillations per course of treatment.
Read the next article Interstitial cystitis: conservative treatment. Part 2.
Diagnosis of interstitial cystitis
- General urine test and urine culture for flora, which can exclude urinary tract infection
- Gynecological examination in women and digital rectal examination in men to exclude inflammatory diseases of the genital organs, urethral diverticula and the presence of neoplasms.
- Ultrasound of the genitourinary organs is also performed to exclude oncological processes
- Urodynamic study
- Cystoscopy is one of the main methods for diagnosing interstitial cystitis
Cystoscopy is performed under anesthesia. GL Hunner first described, in 1914, a simple bladder ulcer combined with severe inflammation and decreased bladder capacity in patients with intense pain. This is characteristic of interstitial cystitis. However, much more often, up to 90%, ulcerative changes in interstitial cystitis are not detected. Accordingly, depending on the cystoscopic picture, two types of interstitial cystitis are distinguished:
Differences from other types of cystitis
This form of cystitis differs from others in that it is non-infectious. In this case, the signs are typical for the pathology in general, but the symptoms are extremely vivid.
Due to metabolic disorders and other problems of the body that occur against the background of cystitis, the disease threatens with severe complications that lead to a sharp decrease in the quality of life and even disability.
Types of interstitial cystitis
- Ulcerative interstitial cystitis with the presence of Hunner's ulcer
- Nonulcerative interstitial cystitis
The appearance of diffuse foci of petechial, submucosal hemorrhages - glomerulations and ruptures of the bladder mucosa with waterfall-type bleeding in more than two cystoscopic fields of view are criteria for confirming interstitial cystitis in the absence of Hunner's ulcer. A bladder biopsy is the final part of cystoscopy for interstitial cystitis. A multifocal biopsy is performed, taking several tissue samples from the bladder wall. Histological examination allows us to exclude a tumor, document the presence of inflammation of the bladder wall, its severity and the cellular composition of the infiltrate.
Classification of the disease
There are two types of interstitial cystitis:
- Ulcerative . In place of the destroyed mucous and submucosal layer, a so-called Hunner's ulcer appears - a place of inflammation. It is considered a classic type of pathology. If during examination specialists discover an ulcer, there is no doubt about the diagnosis.
- Non-ulcerative . The inflammatory process mainly occurs in the submucosa, so there are no signs on the mucosa. Accordingly, it is extremely difficult to establish an accurate diagnosis without additional research methods.
The non-ulcer type of the disease occurs in 70% of cases.
Treatment of interstitial cystitis
1. Instillation of medications into the bladder. Currently, the drug Uro-Gyal , which restores the surface layer of the bladder, is widely and effectively used. Effective for non-ulcer interstitial cystitis. Instillations are performed under local anesthesia.
2. TUR of the bladder is used for ulcerative interstitial cystitis and in case of ineffective treatment with a course of instillations into the bladder. TOUR of the bladder is performed under spinal anesthesia.
Treatment. How is it going?
The urologist develops a treatment program after a thorough examination of the patient. First of all, medications are prescribed:
- Antihistamines - to eliminate signs of an allergic reaction;
- Antidepressants – for pain relief and improvement of psycho-emotional state;
- Mucopolysaccharides - to normalize metabolism, restore the mucous and submucosal layer.
Such therapy reduces pain and partially normalizes the outflow of urine. However, the most effective is the introduction of drug complexes directly into the bladder.
Medicines act directly on damaged organ walls. Urologists perform instillations - drip administration of medications directly into the area of inflammation. Doctors use complexes that contain painkillers that restore mucous membranes, accelerate healing, and eliminate inflammation.
Additionally, physiotherapy is prescribed: exposure of tissue to waves and sounds of different frequencies. When the main symptoms are relieved, so-called bladder gymnastics, massages, and physical therapy courses are performed. The methods are aimed at restoring blood circulation in the pelvic area.
If treatment does not produce results, urologists prescribe operations to excise the affected tissues with further stitching of already functional ones. If the damage is severe, plastic surgery is chosen - organ tissue is replaced with synthetic materials.