Overview of Ocular Hypertension
The term “ocular hypertension” most often refers to any situation in which the pressure inside the eye, i.e. intraocular pressure is higher than normal. Eye pressure is measured in millimeters of mercury (mmHg). The norm is pressure from 10 to 21 mm Hg. Art. Ocular hypertension occurs when eye pressure is higher than 21 mm Hg. Art.
Ocular hypertension is defined by the following criteria:
- Intraocular pressure is more than 21 mmHg. Art. measured using a blood pressure monitor during two or more visits to the doctor;
- The optic nerve is normal;
- The absence of signs of glaucoma is detected during a practical vision test that evaluates peripheral (or side) vision.
To determine other possible causes of high eye pressure, an ophthalmologist (a doctor who specializes in treating eye diseases) will determine whether the system that removes fluids or other secretions is blocked. For this, a method called gonioscopy is used. Gonioscopy involves using special contact lenses to check how open, closed, or narrowed the eye's secretory ducts are. No signs of any eye diseases. Some of these diseases can increase intraocular pressure.
Ocular hypertension should not be considered as a separate disease. This term applies to people who should undergo a more thorough examination in the early stages of glaucoma. A person with ocular hypertension may be suspected of having glaucoma. An eye test can reveal the optic nerve affected by glaucoma.
As previously mentioned, increased intraocular pressure can have other causes. However, for the purposes of this article, ocular hypertension refers primarily to increased intraocular pressure without loss of vision or any damage to the optic nerve. Glaucoma occurs when there is high intraocular pressure, damage to the optic nerve and loss of vision.
Studies using existing tests indicate that 3-6 million people, including 4-10% of the population over 40 years of age, have an intraocular pressure of 21 mmHg. Art. or higher without evidence of glaucomatous damage. Research over the past 20 years is helping to identify the characteristics of people with ocular hypertension.
Recent data from the Ocular Hypertension Study showed that people with ocular hypertension have an average 10 percent risk of developing glaucoma within five years. The risk can be reduced by up to 5% if eye pressure is lowered with medication or laser surgery. However, the risk may be reduced to less than 1% per year due to greatly improved methods for detecting glaucomatous damage. These methods may allow treatment to begin before blindness occurs. Future studies will help further determine the risk of developing glaucoma.
How often should you have your eyes checked?
Patients with thin corneas may be at risk for glaucoma, so the ophthalmologist may use a special device called a pachymeter to measure the thickness of the cornea.
The likelihood of developing ocular hypertension is 10-15 times higher than the occurrence of primary open-angle glaucoma, its common form. This means that out of 100 people over 40 years old, about ten of them will have a blood pressure higher than 21 mm Hg. Art., but only one will develop glaucoma.
Over a 5-year period, several studies have shown that the incidence rate of glaucoma in people with ocular hypertension is approximately 2.6-3% for intraocular pressure of 21 to 25 mmHg. Art., 12-26% for pressure from 26 to 30 mm Hg. Art., and approximately 42% for pressure above 30 mm Hg. Art.
In about 3% of people with ocular hypertension, the veins in the retina may become blocked (called retinal vein occlusion), which can lead to vision loss, so people with ocular hypertension and those over 65 are often advised to keep the pressure below 25 mmHg. Art.
Some studies have found that the eye pressure of African Americans is, on average, higher than that of white people, while in other studies, researchers have found no obvious difference.
Although some studies show that women have higher intraocular pressure on average than men, other studies do not report such a difference.
Some studies suggest that women may have a higher risk of ocular hypertension, especially after menopause.
Studies also suggest that men with ocular hypertension may have a higher risk of glaucomatous damage.
With age, intraocular pressure increases and the risk of glaucoma increases. After 40 years, there is a huge risk of developing both ocular hypertension and primary open-angle glaucoma.
High blood pressure in young people is a cause for concern. Throughout their lives, young people are often exposed to high blood pressure and are more likely to suffer optic nerve damage.
Back to contents
Why is tonometry performed?
The anterior chamber of the eye, which is limited in front by the cornea, along the back wall by the lens and iris, is filled with a special liquid (aqueous humor).
The fluid (secretes from 3 to 9 ml per day) constantly moves, performing the function of nourishing and protecting avascular structures (lens, cornea), when it stagnates, intraocular pressure increases, while at the beginning of the development of the pathology the symptoms are very scarce.
Tonometry of the eye makes it possible to recognize the onset of changes in time and prevent the development of glaucoma (optic nerve atrophy, which leads to irreversible loss of vision).
Causes of ocular hypertension
What is target intraocular pressure?
Increased intraocular pressure is a cause for concern for people with ocular hypertension, as it is one of the main factors in the development of glaucoma .
High pressure inside the eye is caused by an imbalance in the production and removal of fluid from the eyes (aqueous humor). As a result, more and more fluid begins to be produced, causing an increase in pressure.
Imagine a balloon that is filled with water. The more water is poured, the larger the ball becomes. The same with excess intraocular fluid: the more there is, the higher the pressure. If the balloon is filled with too much water, it may burst. High blood pressure due to excess fluid can damage the optic nerve.
Back to contents
Classification
Ocular hypertension has many development options. According to etiology, the disease is classified into uveal, reactive and steroid forms. From a clinical point of view, there are:
- Symptomatic ocular hypertension
. A temporary increase in IOP develops against the background of a pathological process that is not related to glaucoma. - Essential ocular hypertension
. It is characterized by a slight increase in ophthalmotonus with normal levels of intraocular fluid outflow. - Pseudohypertension of the eye
. This is an increase in intraocular pressure that occurs as a result of stress before visometry in healthy people.
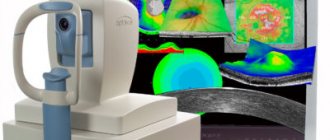
Examinations and tests
Find out more about tonometry
An ophthalmologist performs tests to measure intraocular pressure to treat early stages of glaucoma or its secondary causes.
These analyzes are described below:
- First, visual acuity (how well a person can see objects around them) is assessed. To do this, the patient is asked to read the letters from the optometric table from a considerable distance.
- The cornea, anterior chamber of the eye, iris and lens of the eye are examined under a special microscope - a slit lamp.
- Tonometry is a method used to measure intraocular pressure. Measurements are taken from both eyes in 2-3 sessions. This may happen at different times of the day (such as during the day or evening) as the pressure inside the eye changes every hour. The difference in pressure in both eyes is 3 mmHg. Art. or more may suggest glaucoma. There is a high likelihood of early primary open-angle glaucoma if intraocular pressure increases.
- The optic nerves are checked for any damage or abnormalities through checking dilated pupils. For further information and comparison, a color photograph of the fundus is taken, which captures the image of the optic nerve head (its anterior surface).
- Gonioscopy is performed to check the excretory canal of the eyes using special contact lenses. This test is important to determine how open, narrowed or closed the channels are and to eliminate any other causes of increased intraocular pressure.
- The visual field assessment procedure tests peripheral (or side) vision, usually using an automated visual field testing machine. The test is done to correct any visual field defects caused by glaucoma. It is possible that a repeat procedure may be required. If there is a small risk of glaucomatous damage, then it is worth checking only once a year. If the risk is high, then the test must be done every 2 months.
- Pachymetry (or corneal thickness) is measured using an ultrasound probe to determine the accuracy of intraocular pressure readings. A thin cornea can give a falsely low pressure reading, while a thick cornea can give a falsely high pressure reading.
Back to contents
Symptoms of ocular hypertension
Hemorrhoids kill the patient in 79% of cases
The clinical manifestations of the pathology are determined by the development variant. Essential ocular hypertension is characterized by a stable or regressive course. This is due to the fact that with age, the intensity of intrauterine fluid production gradually decreases. In most cases, ocular hypertension occurs symmetrically in both eyes. Patients report frequent headaches. The exception is the symptomatic form against the background of a glaucomocyclic crisis. With this pathology, one eye is affected. During a crisis, patients complain of discomfort, the appearance of “fog” and rainbow circles before the eyes. There is usually no pain syndrome.
With the steroid type of the disease, intraocular pressure increases gradually. In the reactive version, signs of ocular hypertension increase over 2-6 hours after injury or surgery. Patients complain of a foreign body sensation, blurred vision, and severe pain. Dyspeptic manifestations (nausea, vomiting) are rarely observed. Specific symptoms of the uveal form include ocular hyperemia, photophobia, and increased lacrimation. The disease can lead to irreversible loss of visual function.
Therapeutic treatment
The goal of therapeutic treatment is to lower the pressure before it causes glaucomatous vision loss. This treatment is used for people at greatest risk of developing glaucoma and people with optic nerve damage.
The method of treating the patient is selected individually by the ophthalmologist. Depending on the situation, a person may undergo a course of medication or simply be monitored. The doctor will discuss with the patient the pros and cons of treatment and examination:
Some ophthalmologists use local treatment to lower intraocular pressure above 21 mmHg. Art. Others do not prescribe treatment until optic nerve damage is confirmed. Most prescribe treatment if the pressure rises above 28-30 mm Hg. Art. due to the high risk of damage to the optic nerve. The ophthalmologist will begin treatment if the patient has symptoms such as blurred vision, pain, or intraocular pressure continues to increase on subsequent visits.
Intraocular pressure is periodically determined according to the following principles:
- Drug treatment is prescribed if intraocular pressure is 28 mmHg. Art. or higher. After a month of taking the medication, the patient visits an ophthalmologist to ensure that the medication is lowering blood pressure and that no side effects are observed. If the medicine is effective, then re-examination occurs every 3-4 months.
- If intraocular pressure is 26-27 mm Hg. Art., re-examination occurs 2-3 weeks after the first visit. If during the second visit the difference in pressure readings is within 3 mm Hg. Art., then subsequent examinations occur every 3-4 months. If during the second visit the pressure is lower, then the interval between subsequent visits is determined by the ophthalmologist. At least once a year, the patient should undergo a visual field test and an examination of the optic nerves.
- If intraocular pressure is 22-25 mmHg. Art., a repeat visit occurs after 2-3 months. If during the second visit the difference in pressure readings is within 3 mm Hg. Art., then the next examination occurs after 6 months and includes undergoing a procedure for checking the visual field and checking the condition of the optic nerves. The examination is repeated at least once a year.
Repeat visits may also be scheduled for the following reasons:
- If any defect is detected during the visual field test, repeated (possibly multiple) examinations occur. The ophthalmologist carefully examines the defect, as it may be a sign of early primary open-angle glaucoma. This is why it is important to do your best during the procedure, as this may determine whether you should start taking medications that lower intraocular pressure. If the patient is tired during the procedure, he should tell the specialist to pause the test: this way the person can rest. This will allow you to get a more accurate result.
- Gonioscopy is performed at least once every 1-2 years if intraocular pressure increases significantly or the patient is taking miotics (a type of glaucoma medication).
- If the appearance of the optic nerve or optic disc changes, more color photographs of the fundus (photographs of the back of the eye) are taken.
Medicines
An ideal drug for ocular hypertension should effectively lower intraocular pressure, have no side effects, and be inexpensive. However, there is no such ideal medicine. When choosing medications, the ophthalmologist prioritizes qualities based on the specific needs of the patient.
Medicines, usually in the form of eye drops, are prescribed to reduce high intraocular pressure. Sometimes you need to take more than one medicine.
To test the effectiveness of eye drops, you can first drop them into only one eye: if there are no side effects, your doctor will prescribe them.
Along with taking medications, regular visits to the ophthalmologist are prescribed. Typically, the first examination occurs 3-4 weeks after starting medication.
The ophthalmologist checks your blood pressure to make sure the medicine is helping. If there are no side effects, then the treatment continues, and a re-examination occurs after 2-4 months. If the medicine is ineffective, then another one is prescribed. The doctor may order examinations depending on the medications taken, since some of them (for example, latanoprost [Xalatan], travoprost [Travatan], bimatoprost [Lumigan]) may show results only after 6-8 weeks of use.
During examinations, the ophthalmologist may also examine the patient for any allergic reactions. If a patient experiences any side effects while taking medication, they should tell their doctor.
In general, if intraocular pressure does not decrease after taking 1-2 medications, the patient may have early primary open-angle glaucoma rather than ocular hypertension. In this case, the ophthalmologist may suggest other treatment methods.
Surgical intervention
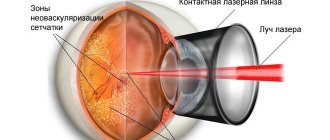
Learn more about laser trabeculoplasty
Laser and surgical treatments are not typically used to treat ocular hypertension because the risks associated with these methods are greater than the risk of developing glaucomatous damage from ocular hypertension. However, if medication is not an option, laser surgery may be an alternative, but this is best discussed with your ophthalmologist.
Next steps
Depending on the extent of optic nerve damage and the status of intraocular pressure readings, people with ocular hypertension should be examined every 2 months, even sooner if pressure is not well monitored.
Glaucoma should be a concern for people who have high intraocular pressure but the optic nerves and visual field test results are normal, and people who have normal intraocular pressure but the optic nerves and visual field test results are questionable. These people should undergo a thorough examination: they are at increased risk of developing glaucoma.
Back to contents
Diagnostics
In the eye clinic on Kurzenkov, the diagnosis of “ophthalmohypertension”, in the absence of obvious causes, is established only after excluding primary glaucoma. To do this, a standard set of diagnostic tests is carried out to identify glaucoma, which includes:
- Visometry and perimetry with testing of visual acuity and its fields;
- Ophthalmoscopy – examination of the condition of the fundus of the eye;
- Tonometry (daily) to monitor intraocular pressure in the morning and evening;
- Tonography – determination of the hydrodynamics of the organ of vision;
- Gonioscopy – visual examination of the anterior chamber;
- Loading and unloading tests that change IOP;
- Retinal tomography (HRT) to determine the status of the optic disc.
If there is a suspicion that the cause of ocular hypertension is an extraocular pathology, the patient may be referred to other diagnostic procedures: ultrasound Dopplerography of blood vessels, study of hormonal status, etc. A decisive role in the differential diagnosis of ocular hypertension from initial open-angle glaucoma belongs to dynamic monitoring of the condition of the eyes.
How is eye pressure measured?
At home, the patient can use only one method available to him - palpating the eyeball through the eyelids, determining by touch the degree of its density. If the pressure is normal, then with gentle pressure you should feel a moderately elastic round ball under your fingers. With an increased IOP, it will be quite hard and not prone to deformation, but with a decreased IOP, on the contrary, it will sag. Of course, this method does not give correct readings and can only be used to understand the approximate condition, although people suffering from elevated IOP acquire the necessary skills over time. The exact data can be found in the doctor’s office, where he will conduct an examination using special instruments and also examine your fundus.