BRIEFLY ABOUT KIDNEYS.
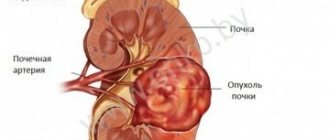
The kidneys are two bean-shaped organs located on the back of the abdominal cavity. Each bud is approximately the size of a fist. The lower ribs of the chest protect the kidneys from injury.
The main function of the kidneys is to filter the blood and rid the body of excess water, salt and waste products in the urine. Urine is removed from the kidneys through the ureter, which drains into the bladder, where urine accumulates until urination. The patient can live with only one kidney.
Nephroblastoma (Wilms tumor) is the most common type of malignant kidney tumor in children. The tumor is named after the German physician Max Wilms, who first described it in 1899.
Nephroblastoma usually affects one kidney. However, 5% of patients may have bilateral involvement.
Most nephroblastomas are diagnosed only when they reach large sizes, although they have not yet metastasized (spread) to other organs. The average weight of a nephroblastoma is about 500 grams, which significantly exceeds the weight of a normal kidney.
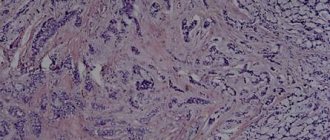
After a biopsy or removal of the affected kidney, the tumor tissue is examined under a microscope. There are two main types of nephroblastoma:
- Nephroblastoma with favorable histological structure
- Nephroblastoma with unfavorable histological structure
In tumors with an unfavorable histological structure, the nuclei (the central part of the cell containing DNA) of the tumor cells are very large and altered, this condition is called anaplasia. The more pronounced the symptoms of anaplasia, the worse the outcome of the disease.
A favorable histological structure means the absence of signs of anaplasia and a good prognosis. In 95% of cases, a favorable histological structure of nephroblastoma is revealed.
Answers to frequently asked questions
Will a child be able to live with one kidney after surgery?
If the Wilms tumor affects only one kidney, then after its removal the child grows and develops completely normally, because the second one is fully functioning. For bilateral nephroblastoma, doctors will find an organ donor.
How to suspect a tumor in a child?
The first symptoms appear between the ages of 6 months and 5 years. They are nonspecific - lethargy, poor appetite, blood tests show an increase in ESR and a decrease in hemoglobin levels. Therefore, it is important to monitor the child’s health, undergo regular medical examinations with a pediatrician, and at the first sign of trouble, look for its cause.
OTHER TYPES OF KIDNEY TUMORS.
About 90% of kidney tumors in children are nephroblastomas, while in adults nephroblastoma is extremely rare. Almost all malignant kidney tumors in adults are renal cell carcinomas, which are very rarely diagnosed in children.
Other rare tumors that may be diagnosed in children include mesoblastic nephroma, clear cell sarcoma, and malignant rhabdoid tumor.
If these rare kidney tumors in children reach large sizes and extend beyond the kidneys, the prognosis of the disease is poor. These tumors are treated more intensively compared to nephroblastoma.
Symptoms
The danger of nephroblastoma lies in the asymptomatic course of the disease for too long. With a small tumor size, classical ultrasound equipment does not allow recognizing the first signs of neoplasia - the beginnings of focal changes in the structure of the renal tissue.
At the initial stage, kidney nephroblastoma in children is most often unilateral, and as the pathology progresses, certain symptoms appear:
- asymmetry of the abdomen, unilateral increase in volume;
- palpation of the tumor;
- the appearance of blood in the urine (hematuria), as a sign of tumor growth into the renal pelvis;
- severe pain during tumor growth;
- when the tumor grows excessively, nephrotic syndrome .
As the disease progresses, signs of chronic renal failure . With metastasis , characteristic clinical symptoms of the affected organs appear.
Episodic hyperthermia , an increase in body temperature without signs of acute respiratory viral infections and respiratory infections, is also recorded. Parents complain of moodiness, regular regurgitation of fresh milk, bowel irregularities, general malaise, and signs of intoxication .
Risk factors for nephroblastoma
A risk factor is something that increases your chance of developing cancer. There are different risk factors for different tumors. These may include genetic (inherited) factors, as well as environmental and lifestyle factors. In general, lifestyle factors (smoking, poor diet and physical inactivity) are the most important factors in most adult malignancies. However, they have little, if any, effect on the risk of tumors in children.
Environmental risk factors.
No relationship was found between nephroblastoma and environmental factors either before or after the birth of the child.
Genetic and inherited risk factors.
Cases of nephroblastoma in the family. 1-3% of children with nephroblastoma have one or more relatives who have suffered the same disease. It is assumed that these children inherited an altered gene from one of the parents, which significantly increases the risk of nephroblastoma. Patients with familial cases of nephroblastoma, compared with sporadic tumors (without the presence of relatives with a similar tumor), are more likely to develop bilateral kidney damage.
The presence of certain birth defects . There is a clear relationship between nephroblastoma and certain birth defects. Thus, 15% of children with nephroblastoma have birth defects, most often represented by syndromes. A syndrome is several symptoms, signs, malformations or other disorders that occur in the same patient.
WAGR syndrome : Aniridia (complete or partial absence of the iris, disorders of the genitourinary tract (defects of the kidneys, penis, scrotum, clitoris, testicles or ovaries), mental retardation. Patients with such developmental defects have a 3% chance development of nephroblastoma.
Beckwith-Wiedemann syndrome : Presence of large internal organs, especially the tongue. Hemihypertrophy (an increase in the size of one arm or leg on one side of the body) is possible. These people are more likely to develop nephroblastoma.
Denis-Drash syndrome : Underdevelopment of the penis, testicles and scrotum. For this reason, boys with this syndrome may be mistaken for girls. For some unknown reason, the kidneys in such children begin to function poorly or stop functioning altogether. Nephroblastoma can occur in these altered kidneys.
There are a number of other rarer syndromes associated with nephroblastoma.
Gene and chromosomal changes in children with birth defects and nephroblastoma . Genes determine eye and skin color, blood type, etc. Changes in the DNA of a gene can lead to the development of the disease. Changes in DNA are called mutations. Sometimes these mutations are inherited from parents. This explains the fact that some diseases are more common among members of the same family.
Genes are part of chromosomes, which are giant DNA molecules containing thousands of genes. DNA is contained in 23 pairs of chromosomes. One gene from each pair is inherited from the mother and one from the father.
The previously mentioned syndromes are associated with deletions (missing part of DNA) or mutations of genes on chromosome 11.
List of sources
- Karavaeva E.A., Taranushenko T.E., Morgun A.V., Borisova M.V., Kadricheva T.G., Bulava T.I., Gonchar N.A., Guseinova E.A. “Renal tumors in children and adolescents (primary diagnosis according to a pilot study)”, Breast Cancer. Mother and child No. 2 from 31.05; 2021.
- Zheludkova O.G., Polyakov V.G., Rykov M.Yu. and others. “Clinical manifestations of cancer in children. Practical recommendations" St. Petersburg, 2021.
- Vasilyeva T.A., Voskresenskaya A.A., Kadyshev V.V., Pozdeeva N.A., Marakhonov A.V., Zinchenko R.A. “Clinical-molecular-genetic features of congenital aniridia”, RMJ, 2021.
What causes nephroblastoma?
Although there is a clear link between nephroblastoma, birth defects, and genetic mutations, most children with this tumor do not have any birth defects or inherited genetic changes.
The cause of nephroblastoma in children is not yet understood, but significant progress has been made in understanding many of the events that occur during the formation of normal fetal kidneys and how this process is altered to lead to nephroblastoma.
Kidneys develop very early in the womb. Sometimes defects may occur during their development. Some cells that should turn into mature kidney cells do not do this and remain embryonic (fetal, or early). Some clusters of these early kidney cells may exist for a period of time after the baby is born. Typically, these cells mature by the age of 3-4 years. If this does not happen, the cells may begin to grow uncontrollably. The result of this process is the development of nephroblastoma. Having a mutation or deletion of the WT1 or WT2 genes increases the risk that some cells will remain embryonic and lead to the development of nephroblastoma.
How common is nephroblastoma?
In the structure of malignant tumors in children in Russia, nephroblastoma ranks 4th (6%), behind tumors of the hematopoietic and lymphatic systems (40%), tumors of the central nervous system (15%) and soft tissue sarcomas (8%). Its frequency ranges from 0.4 to 1 per 10 thousand newborns.
In the United States, almost 500 new cases of nephroblastoma are diagnosed annually, and this number has remained constant for many years. Nephroblastoma most often occurs in young children. As the child's age increases, the frequency of detection of nephroblastoma decreases. After 6 years the tumor is rare. Nephroblastoma is detected somewhat more often among African Americans and girls.
Non-Hodgkin's lymphomas
A tumor of the lymphatic tissue with possible spread of the process to the hematopoietic and any underlying tissue. There is no age peak; children under 2 years of age rarely get sick. Boys get sick 3-5 times more often than girls. In Burkitt's lymphoma, the etiological factor is Epstein-Bar virus.
The main predominant primary localizations: in the abdominal cavity and organs of the gastrointestinal tract, peripheral lymph nodes, lymph nodes of the mediastinum, pharyngeal ring. The clinical manifestations depend on the location of the tumor. At the onset of the disease, general weakness, decreased performance at school, and pale skin. Further clinical picture of acute abdomen, pleurisy, enlarged peripheral lymph nodes. According to many experts, parents do not pay attention to the enlargement of the lymph nodes and carry out thermal procedures (for malignant lesions, any physiotherapeutic procedures contribute to the generalization of the process). Diagnosis and treatment are similar to lymphogranulomatosis.
Is early detection of nephroblastoma possible?
Children with birth defects associated with the possibility of nephroblastoma should be monitored and undergo special examination. Ultrasound examination (ultrasound) should be performed every three months until the child reaches 6-7 years of age in order to early recognize a kidney tumor, when it has not yet spread to other organs. It is necessary to inform your doctor about the presence of a relative with nephroblastoma in your family and examine him. all other children of the family with regular ultrasound examinations.
Given the rarity of nephroblastoma, there is no need to recommend ultrasound as a screening method (the use of any test in people without signs and symptoms of the disease), unless, of course, the child has risk factors for developing nephroblastoma.
How is nephroblastoma diagnosed?
Nephroblastoma is sometimes difficult to detect in the early stages because it often reaches large sizes without causing pain in the child. Children with such a tumor may appear quite healthy and lead a normal life. Usually the first sign of the disease is an increase in the size of the abdomen. Parents may notice an enlarged abdomen or tumor formation in it while washing and dressing the child. Up to 25% of people with nephroblastoma may experience abdominal pain, fever, blood in the urine, or increased blood pressure. If your child has any of these symptoms, you should consult a doctor immediately.
SURVEY METHODS.
Modern examination methods include computed tomography (CT) , magnetic resonance imaging (MRI) and ultrasound (US) and play an extremely important role in the diagnosis of most types of kidney tumors.
Ultrasound . This method uses sound waves to produce images of internal organs. At the same time, the tissue of a healthy kidney differs from the tissue of a tumor, and benign tumors from malignant ones.
This method is used primarily in cases of suspected nephroblastoma, as it is a painless procedure that allows you to examine the entire abdomen.
CT scan . The method allows you to obtain multiple detailed transverse images of the body and identify kidney tumors. Simultaneous injection of a contrast agent into a vein makes it possible to have a clearer picture of the area being examined.
CT is one of the most effective methods for detecting a tumor inside the kidney, as well as its spread outside the organ. The lungs are the most common site of metastasis in nephroblastoma.
Spiral CT is a new and improved method for detecting small lesions within the kidney, which also uses intravenous contrast.
MRI (magnetic resonance imaging) . This method uses radio waves and strong magnets, which allow a more detailed study of the organ and the vessels involved in the process compared to CT.
Angiography . During this procedure, a contrast agent is injected into the artery, which helps to better view the vessels, including those leading to the kidneys, which is extremely important for the surgeon when planning surgery.
Chest X-ray can detect lung damage due to nephroblastoma.
Bone scan . A radioactive substance injected into a vein accumulates in the area of bone tissue damage, which is detected using a special device. The dose of radioactive substance administered is minimal and not harmful to the child.
Neuroblastoma
They arise from the fibers of large nodes of the sympathetic nervous system, located in the walls of the internal organs, the adrenal medulla. They account for 6% of all malignant tumors in children. 1 child per 100,000 people gets sick. Most common in young children.
The most common locations are retroperitoneal (adrenal glands and paraganglia) and posterior mediastinum. At the beginning of the disease, loss of appetite, lethargy, tearfulness, pale skin, low-grade fever. When palpating the abdomen in the upper and middle parts of the abdomen, a slow-moving and lumpy tumor (unlike nephroblastoma) is palpated, and sometimes ascites is detected. However, clinical signs are often caused by metastases. With metastases to the bones of the skull, tumor-like tubercles are detected in the forehead, scalp, and exophthalmos. Most often metastases to the bone marrow.
For early diagnosis of the disease it is necessary to:
— Ultrasound of the abdominal cavity and retroperitoneal space;
— RCT, MRI of the abdominal cavity;
— RCT of the chest organs;
- MIBG
- blood for tumor markers (NSE, ferritin), urine (catecholamines).
- puncture of the formation with cytological examination.
After the diagnosis is established, complex treatment is carried out: polychemotherapy, surgery, depending on the risk group, radiation therapy, MIBG therapy.
You need to know that neuroblastoma can undergo spontaneous regression (self-healing), by turning into a benign neurogenic tumor (ganglioneuroma).
How is the stage of nephroblastoma determined?
The stage of the disease is determined by the extent of tumor spread. The stage of the disease is clarified using various research methods, during surgery and taking into account the study of the removed tumor.
With nephroblastoma, there are 5 stages (from I to V) of the disease. Treatment and prognosis of the disease largely depend on the stage of the tumor.
Stage I nephroblastoma is diagnosed in 41% of cases, II - in 23%, III - in 23%, IV - in 10% and V (damage to both kidneys) - in 5% of cases.
Procedures and operations
For bilateral or extensive lesions, a total nephrectomy (complete removal of the kidneys) is performed. Subsequently, replacement therapy is required:
- transplantation from a cadaveric donor or relative;
- peritoneal dialysis (through an abdominal stoma);
- hemodialysis.
If it is impossible to carry out surgical treatment, palliative care is prescribed, the purpose of which is to constantly maintain the kidney and the child himself in a viable condition. For this purpose, chemical / radiation therapy and syndromic treatment are prescribed.
Treatment of nephroblastoma
More than 90% of children with nephroblastoma make a full recovery. Advances in treatment have been achieved through the use of surgical, radiation and medicinal methods.
After nephroblastoma is detected and the stage of the disease is clarified, a treatment plan is developed.
Taking into account the rarity of nephroblastoma, it is advisable to be treated in specialized pediatric oncology departments, in which doctors have significant experience. Treatment of the child should not be delayed, since nephroblastoma grows very quickly.
Treatment for nephroblastoma includes surgery, chemotherapy, and sometimes radiation therapy. If there is residual tumor after the first operation, radiation therapy and repeat surgery may be required. The main goal of treatment is to remove the primary tumor, even if there are distant metastases, for example in the lungs.
In some cases, the tumor may be too large and involve vital structures, making surgery impossible at the moment. In some patients, the lesion may be bilateral. In these patients, chemotherapy or radiation therapy, or a combination of the two treatments, is first used to shrink the tumor before removing it.
Brain tumors
They account for 16% of all malignant tumors in children. 3-4 children per 100,000 people become ill.
Different tumors have a number of common features. They are located inside the closed space of the skull, influencing the cells of the brain substance. In young children, the earliest sign is an enlarged head with swelling and tension of the springs. This leads to long-term compensation of increased intracranial pressure. Children stop being interested in the world around them, stop playing, and become drowsy. Schoolchildren become irritable, withdrawn, and refuse to eat. With further development of the disease, general cerebral symptoms appear: paroxysmal bursting headaches, nausea, vomiting in the morning, impaired gait, coordination of movements, convulsions, mental disorders. Clinical signs are associated with the location of the tumor in the brain.
For early diagnosis of the disease it is necessary to:
- X-ray of the skull;
— MRI of the brain with intravenous contrast;
- spinal puncture;
— electroencephalography.
The main type of treatment is surgery, also radiation therapy, chemotherapy, depending on the type of tumor (medulloblastoma, ependymoma, ATRO). Treatment results depend on early diagnosis and radical surgical intervention.