Live broadcasts on Instagram every Sunday at 12:00
Subscribe so you don't miss out! Subscribe
- home
- Oncology
- Kidney cancer
- Author's treatment methods
Kidney tumors can be of either benign or malignant origin. Ranking third among oncological pathologies of the genitourinary system, the disease mainly affects people over 40 years of age, and there are 2 times more patients among men than among women.
There are various options for malignant transformation of renal tissue. Often, kidney cancer remains asymptomatic for a long time. The latent course of the disease makes diagnosis difficult, but even with late detection one can count on a favorable outcome.
The issues of the occurrence, development and treatment of kidney tumors are described in more detail in the corresponding section of this site.
To determine the type of kidney tumor, its localization to the main structures of the organ and indications for surgery, as well as choosing the correct surgical treatment tactics, you need to send me a complete description of the kidney ultrasound, MSCT data of the kidneys with contrast, indicate your age and main complaints to your personal email address. Then I will be able to give a more accurate answer to your situation.
Main symptoms
For a long time, the disease can be asymptomatic. Over time, symptoms appear, the main ones being hematuria (blood in the urine), palpable swelling in the abdomen and pain. Hematuria usually appears suddenly and is short-term. Worm-shaped blood clots can often be found in the urine. You can palpate a tumor only if its size reaches 5 cm, but in overweight patients this is difficult to do even if the tumor is large. The pain is dull in nature and is noted on the affected side. In addition, the person is worried about weakness, fever, and arterial hypertension. As a result of compression of the inferior vena cava, swelling of the legs, dilation of the saphenous veins of the abdominal wall, and varicocele develop. When metastases spread to distant tissues and organs, symptoms characteristic of damage to a particular organ appear: cough and hemoptysis when the lungs are affected, pathological fractures and pain in the bones, jaundice when cancer cells spread to the liver, etc.
K. V. Puchkov: “Oncological disease is not a death sentence”
Free consultation with a urologist
A simple renal cyst is a benign formation, usually detected as an incidental finding during computed tomography or ultrasound examination of the retroperitoneal organs. Despite the fact that most often a person may not even know about the existence of a simple kidney cyst and may not have any symptoms of the disease, if complications of the kidney cyst develop, diagnosing the disease is often extremely difficult. In addition, it should be noted that in 2% of cases there is “coexistence” of both a simple kidney cyst and carcinoma (cancer) in the same kidney.
A simple kidney cyst is a round formation filled with clear fluid and has no communication with the renal collecting system. It is called a simple renal cyst because it consists of a single chamber (cavity), in contrast to multi-chamber cysts. In most cases, a simple kidney cyst is a unilateral phenomenon, i.e. one kidney is affected. However, there are cases where a patient has several simple kidney cysts or cysts appear on both kidneys. A simple cyst is usually located on the surface of the kidney.
A simple kidney cyst can form in any part of the kidney, however, according to the literature, in most cases the kidney cyst is located in the region of the lower pole of the kidney. A simple cyst does not affect the size of the kidney, unlike other cystic diseases, such as polycystic kidney disease. Sometimes a simple kidney cyst can be located in the deep layers of the kidney, i.e. not on its surface, while the wall of the cyst is adjacent to the wall of the renal pelvis or renal calyces and is difficult to separate from them. The size of a simple kidney cyst can vary from a few millimeters to ten or more centimeters in diameter. Let us once again draw attention to the fact that a simple kidney cyst has a very thin wall, lined with single-layer cubic epithelium, and inside the cyst there is never any other content other than liquid. Simple kidney cysts belong to category I according to the Bosniak classification. The risk of malignancy of a simple kidney cyst, according to various sources, ranges from zero to two percent.
A type of simple renal cyst is a hyperdense renal cyst. A hyperdense renal cyst is a simple renal cyst containing blood. Such a cyst is called hyperdense because on computed tomography it has a higher density than a simple kidney cyst. Such kidney cysts can also be called hemorrhagic. Hyperdense renal cysts belong to category II according to the Bosniak classification (benign, minimally complicated renal cysts). The risk of malignancy in hyperdense renal cysts is also low.
Simple kidney cysts are quite common and in most cases occur in older people. The incidence of cysts increases with age: 20% of people aged 40 years have simple kidney cysts, while in people over 70 years of age this pathology occurs in 30% of cases. According to the results of many studies, the size and number of cysts tend to increase with age.
Thus, the main risk factor for developing a simple kidney cyst is age. However, one interesting study found that smoking is also a significant risk factor for the development of simple kidney cysts. According to many studies, simple kidney cysts are more common among men than among women. Some authors explain this fact in this way: a simple kidney cyst is formed due to the expansion of the nephron tubules as a result of obstruction, which is facilitated by the phenomenon of prostatitis in men; Also, a number of authors believe that smoking, which is more common among men, can contribute to the appearance of simple kidney cysts due to a direct toxic effect on the kidneys or the development of renovascular disease.
Simple kidney cysts less than 3 cm in size that do not cause any symptoms do not require treatment, only dynamic observation is necessary. If the cyst increases in size and causes serious symptoms in a person (back pain, increased blood pressure, etc.), the patient should pay special attention to his disease and, by making an appointment with a urologist, discuss possible treatment options with the doctor.
The article is for informational purposes only. For any health problems, do not self-diagnose and consult a doctor!
Author:
V.A. Shaderkina is a urologist, oncologist, scientific editor of Uroweb.ru. Chairman of the Association of Medical Journalists.
‹ Etiology of penile fracture Up Prevention of kidney cancer ›
In what cases is surgery indicated?
Surgery is the main method of treating kidney tumors; a feature of this disease is the lack of sensitivity to radiation and chemotherapy. If untreated, hematuria can provoke the development of anemia; blood clots at a late stage can lead to obstruction of the ureter or tamponade of the bladder, which will cause acute urinary retention. In addition, refusal of treatment for malignant formation means steady progression of the disease. In this case, metastases, spreading throughout the body, affect vital organs: liver, lungs, brain, etc.
Diagnostic methods
First of all, a general clinical examination is carried out, on the basis of which biochemical and cytological studies are prescribed. To clarify the diagnosis, a number of studies are necessary: ultrasound examination, excretory urography, computed tomography.
- Ultrasound - allows you to visualize the deformation of the contours of the kidney, the presence of areas of necrosis and hemorrhages; under ultrasound control, you can perform a targeted puncture biopsy for histological examination of tissues.
- Excretory urography and renal angiography make it possible to differentiate a malignant formation from a cyst, detect a small tumor, a tumor thrombus, and the presence of metastases.
- Magnetic resonance (MRI) and computed tomography (CT) is a study that produces layer-by-layer images of tissue. Thanks to the minimal thickness of the sections, it is possible to detect even minor pathological changes in the kidneys. For greater efficiency, studies are carried out using a contrast agent.
Diagnosis of kidney cancer using CT
CT is the “gold standard” for imaging malignant kidney tumors. Using CT, one can reliably differentiate between a kidney tumor and various types of renal cysts. A prerequisite for reliable diagnosis of tumors is intravenous contrast (CT with contrast enhancement), with which you can clearly visualize the solid, soft tissue part of the formation. In the excretory phase, it is possible to assess how much the tumor deforms the pyelocaliceal complex and impedes the outflow of urine.
Get a kidney CT scan in St. Petersburg
HOW TO PREPARE FOR A KIDNEY CT WITH CONTRAST?
To ensure that kidney tomography does not cause harm, before the study it is necessary to examine the blood to assess excretory function. In a biochemical blood test, the values of creatinine (no more than 110 µmol/l) and urea (no more than 9 mmol/l), as well as the glomerular filtration rate, are important. Exceeding these indicators indicates impaired renal function and is a factor that significantly increases the likelihood of side effects of iodine-containing contrast agents. It is also necessary to make sure that you do not suffer from a pathology of the thyroid gland, accompanied by its increased function (hyperthyroidism, thyrotoxicosis).
Two days before the study, you must adhere to a diet that excludes meat products, especially fatty meats, gas-forming products - legumes, cabbage, etc. On the day of the study, a light breakfast is acceptable. Immediately before the test, it is better not to eat for 2-3 hours. All this is necessary in order to reduce the number of artifacts from intestinal contents and gas. After the study, you need to drink as much fluid as possible, because... contrast agents are eliminated by the kidneys, and drinking plenty of water helps flush them out of the body faster.
You need to take with you all the information regarding your disease, including the results of previous studies (MRI, ultrasound, etc.), as well as an outpatient card and other medical documents. Do not forget the results of blood tests for creatinine and urea.
WHAT HAPPENS DURING A RIDAL CT WITH CONTRAST?
The patient lies down on the tomograph table. Then a catheter is inserted into the vein of the elbow and fixed with a plaster. A special device is connected to the catheter through a thin plastic tube - an automatic injector, into the flask of which a contrast agent is poured.
The scan begins with the native phase, in which no contrast is administered. After this, the laboratory assistant sends a signal to the injector and it begins to administer the contrast, almost simultaneously the second scan begins, during which the arteries, arterioles and capillary vascular bed are filled with contrasted blood. This phase is called arterial-parenchymal, because not only arteries are contrasted, but also parenchymal organs, as well as the wall of hollow organs. During the portal-venous phase, the portal vein, as well as other large veins, strengthens. And finally, in the delayed phase, the pyelocaliceal complex of the kidneys and ureters, as well as the bladder, are filled with contrast - it becomes possible to assess the degree of deformation of the renal cavities by the tumor.
WHAT DOES KIDNEY CANCER LOOK ON CT WITH CONTRAST?
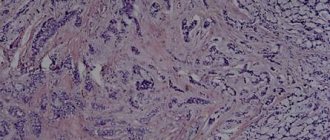
Kidney cancer (hypernephroma, clear cell cancer) can be defined as a node with uneven edges, having a heterogeneous structure with multiple areas of decay, necrosis, soft tissue and liquid components in the structure, presented in various proportions. In addition, in the structure of the tumor node - not in all cases, but often - calcifications and hemorrhages are detected. The size of the node can be very different - from a few mm to 10 cm (or more). Small nodules are often not visible on a non-contrast CT scan and only show up as some bulging of the organ outline - they are often missed on a quick scan of the images (which is why a second opinion from a doctor can be helpful).
A typical type of kidney cancer in the native (before contrast) phase. The parenchymal node in the right kidney (in the circle) is clearly visible. Even without enhancement, you can see its heterogeneous structure - with a predominance of the soft tissue component, as well as the presence of less dense areas and calcium inclusions (red arrow).
In the arterial phase, the heterogeneous structure of the tumor becomes clearly visible, since its solid part (the active part of the tumor, well supplied with vessels) intensively intensifies and becomes hyperdense, and the cystic part does not accumulate contrast in any way and remains the same density as in the native phase . In the venous phase, the tumor retains contrast more intensely than the renal parenchyma, as a result of which it appears more hyperdense and denser. In the delayed phase, already 10 minutes after the start of administration, a typical cancer does not accumulate contrast, but the pyelocaliceal system becomes clearly visible - it becomes possible to evaluate its contours for the growth of a tumor inside.
Diagram illustrating the structure of kidney cancer. It shows all the main elements that make up a typical malignant neoplasm. Number 1 indicates the soft tissue basis of the neoplasm - active cancer cells, the so-called. hypernephroma stroma. 2 – hemorrhages. 3 – calcifications in a thickened, pathologically altered wall and stroma. 4 – cystic component (fluid). K – cortical substance, M – medulla, C – calyces, L – pelvis, M – ureter (in this case – pelvic segment). The mass can also be designated as a Bosniak category 4 cyst (see below).
CT signs of kidney cancer (hypernephroma) in the arterial-parenchymal contrast phase. In the images in the top row, a red arrow indicates a neoplasm in the form of a node with a heterogeneous structure, a blue arrow indicates a simple cyst in the region of the lower pole on the right. In the bottom row, the yellow arrow highlights the soft tissue component, which accumulates contrast and is intensely enhanced. Green arrow – cystic component.
It is very important to evaluate the growth pattern of the tumor node and the presence of metastases using CT. The most unfavorable is the infiltrative type of growth, when the tumor destroys surrounding organs, growing into them - symptoms of intoxication increase, treatment lasts as long as the patient lives - it is only palliative. Most often, the tumor of the left kidney grows into the renal fascia (the so-called Gerota's fascia) - anterior or posterior, depending on its location, into the spleen, into the tail of the pancreas, into the adrenal gland, into the splenic vein, into the renal vein. A tumor of the right kidney can also grow into the inferior vena cava. The presence of invasion is an extremely unfavorable sign, when detected, stage 4 according to TNM (international tumor classification) is assigned, and the neoplasm is considered inoperable.
The most common variants of germination (invasion) of hypernephroma of the left kidney. RV – tail of the pancreas, SV – splenic vein, LA – left kidney, RPF – anterior renal fascia, PRF – posterior fascia. Number 1 indicates a tumor growing into the posterior fascia of Gerota (renal fascia), 2 – with invasion of the perinephric tissue, 3 – with invasion of the anterior fascia of Gerota, 4 – with invasion of the tail of the pancreas, splenic vein, anterior renal fascia, 5 – with invasion into spleen, anterior renal fascia.
Variants of germination (invasion) of hypernephroma of the right kidney. P – liver, IVC – inferior vena cava, PV – renal vein, PP – right kidney, PRF – posterior renal fascia, APF – anterior renal fascia. 1 – tumor with growth into the posterior renal fascia, 2 – into the perinephric tissue, 3 – into the anterior renal fascia and into the liver, 4 – into the inferior vena cava (gas can be detected in the vein), 5 – into the renal vein.
Kidney cancer can metastasize, even after removal, to the lungs - this is the most common way. The prognosis is unfavorable. In the lungs, metastases of such tumors look typical - they are solid nodes of various sizes (from 0.5 to 3 cm in diameter), located diffusely in the parenchyma of the lung tissue. Tumor metastasis occurs as follows: by sprouting venous vessels, tumor cells – the so-called. tumor emboli - enter the renal vein, then into the inferior vena cava, from it into the heart (into the right atrium), into the pulmonary trunk, pulmonary arteries of ever smaller caliber and, finally, settle in vessels whose diameter is less than or equal to their size. There they “grow”, forming a secondary tumor node. In addition, hypernephroma often metastasizes to the bones: vertebrae, ribs, iliac bones, and coccyx. They are lytic in nature - they grow, destroying bone tissue. Kidney cancer with metastases to the lymph nodes in the renal hilum, in the perirenal tissue, along the abdominal aorta can also be detected - the prognosis is very serious, but the detection of pathologically altered lymph nodes in itself is not a contraindication to surgery.
The letter “M” in the image marks metastases of kidney cancer to the lungs, the prognosis of which, if detected, is unfavorable. These are typical hematogenous secondary tumor nodes, diffusely located in the pulmonary parenchyma, with a tendency to increase in number and size in the basal regions. The letters also mark the main anatomical structures: C - cardiac cavity, A - aorta, T - trachea, BT - bifurcation (division into bronchi) of the trachea, PB and LB - right and left bronchus, respectively, SVC - superior vena cava.
RENAL CYSTS ON CT: CYST OR CANCER?
Very often, computed tomography reveals formations of a cystic nature - in this case, the question arises - how to distinguish a simple kidney cyst containing only fluid from cancer? Can a kidney cyst develop into cancer over time? Only contrast can help here. For the differential diagnosis of a simple uncomplicated cyst and potentially malignant cysts, the Bosniak classification (1986) was developed, an illustration for it is presented below.
Class 1 according to Bosniak - a simple, uncomplicated cyst with smooth, thin walls, filled with low-density contents, approximately +10...+15 units on the Hounsfield scale. The shape of such a cyst is regular, close to a ball, the most common size is from 0.3 to 5.0 cm. The most important thing is that such a cyst does not enhance with contrast. The percentage of malignancy is extremely low. Typically, such cysts do not require follow-up.
Bosniak class 2 – minimally complicated cyst. Either septa or calcifications in the wall are detected. Does not accumulate contrast. The percentage of malignancy is low. Such cysts need to be monitored by ultrasound (usually every six months to a year) for changes in size.
Bosniak class 3 – a cyst with a tendency to malignancy. May contain blood, septa with calcium deposits, areas of wall thickening. They can accumulate contrast in a limited area. It is recommended to remove such cysts surgically in the absence of contraindications.
Class 4 according to Bosniak - the cyst has a clearly defined soft tissue component in the structure, uneven edges, tuberous contours, and, most importantly, intensively intensifies in the arterial-parenchymal phase. When such cysts are detected, the diagnosis of “kidney tumor” leaves no doubt, and the prognosis is very serious. Surgery is recommended if there are no contraindications.
WHEN SHOULD YOU DO A KIDNEY CT?
In all cases where there are suspicious symptoms, it is necessary to undergo an X-ray tomographic diagnostic examination as soon as possible:
1) Blood suddenly appeared in the urine. Blood in the urine can be not only a sign of prognostically unfavorable cancer of the renal pelvis, but also tumors of other organs of the urinary system (bladder, prostate), as well as a sign of urolithiasis or glomerulonephritis.
2) Pain appeared in the lower back on the right or left. In addition to hypernephroma, these changes can also be a sign of pyelonephritis, an inflammatory kidney disease most often of an infectious nature, or even pyonephrosis, a purulent melting of the organ.
3) Ultrasound examination revealed a formation suspicious for hypernephroma. Typically, symptoms of kidney cancer in both men and women are clearly identified by ultrasound, especially Doppler ultrasound. However, the doctor performing the ultrasound always refers “suspicious” patients to a CT scan in order to confirm or refute the diagnosis of kidney cancer. CT also makes it possible to establish damage to the lymph nodes, nearby organs, as well as metastases to distant organs (lungs and bones).
DIAGNOSIS OF KIDNEY CANCER AT AN EARLY STAGE - CT CAPABILITIES
With computed tomography, a lesion in the kidney of 0.3 cm can be seen if it has a density different from the renal parenchyma. Of course, such lesions are not always correctly interpreted by a radiologist; many of them are completely ignored or are described as “cysts,” especially if there is no suspicion of cancer. After treatment by resection (after removal of part of the kidney along with the cancerous tumor), the prognosis can be very optimistic - the function of the organ suffers minimally, according to many patients, it is possible to maintain a sufficient quality of life. Diagnosis of stage 1-4 kidney cancer by TNM using computed tomography also does not cause problems.
Get a kidney CT scan in St. Petersburg
SECOND OPINION ON KIDNEY CT FOR CANCER
In some cases, the diagnosis of kidney cancer can be controversial. Thus, diagnosing “small” forms of tumors can be difficult. This also applies to cysts with slightly noticeable wall thickening. The question arises - to what category according to Bosniak should they be classified? If to the second, there is a risk of making a mistake - in six months to a year the patient’s tumor node may grow significantly, and it will become inoperable. If to the fourth, there is a risk of removing a relatively healthy area of the kidney and reducing the patient’s quality of life. In some cases, an inexperienced radiologist may miss kidney cancer altogether.
Here, the opinion of an experienced specialist can play a very important role, and re-analysis of the study by an experienced doctor will correct the mistakes of colleagues. Therefore, if you have been diagnosed with kidney cancer, do not rush to despair, but try to find a specialist who can competently interpret the CT results. As a result, you will receive a Second Opinion on CT - a detailed, qualified description of the images performed by an experienced radiologist who is well versed in oncology. You can get such a Second Opinion on CT in the National Teleradiological Network - this service of remote consultations with doctors provides round-the-clock support to patients in complex diagnostic cases.
Vasily Vishnyakov, radiologist
Read more about Second Opinion
Read more about telemedicine
Pavel Popov
Candidate of Medical Sciences, Member of the European Society of Radiologists
Surgery for kidney cancer
Most medical institutions perform open removal of the entire kidney. However, for a small tumor, surgery can be performed while preserving the organ. Of course, if the tumor is large or located in the center, nephrectomy has to be performed - removal. However, in clinics in Europe and the USA, when treating kidney cancer, the “golden” standard is partial resection - removal of part of the kidney along with the tumor. And only if resection is impossible, nephrectomy is performed - removal of the kidney.
| Rice. 1. | Rice. 2. | Rice. 3. |
| Laparoscopic removal of a kidney tumor - resection within healthy tissue, suturing of the renal wound. | ||
STV: Scat. Master class by K. V. Puchkov
When performing minimally invasive surgery for kidney cancer, I always try to preserve the organ by performing laparoscopic resection. In this case, the kidney is isolated from the tissues surrounding it, then, using a special laparoscopic ultrasound sensor, the localization of the tumor in relation to the pelvis and renal vessels is specified (Fig. 1). In a favorable “surgical” situation, a kidney resection is performed - at a distance of 5-8 mm from the tumor, within healthy tissue, the formation is excised with ultrasonic scissors (Fig. 2). To suture the wound, synthetic absorbable threads are used, as well as hemostatic glue made in the USA and the PerClot hemostatic system (Italy), thanks to which the renal wound can be hermetically closed (Fig. 3).
In difficult cases, I use the V-lock suture system (Covidien, Switzerland), which is made of monofilament absorbable polydioxanone thread with notches on it. The notches are oriented in space at a given angle in one direction. This allows the thread to slide freely in one direction and be virtually unmovable in the opposite direction. Such systems fix fabrics using an anchor type and do not require tying knots. When using this suture system, there is a more thorough comparison of the edges of the wound on the uterus (which leads to even better healing) and the speed of suture formation increases by 3-4 times.
In addition, the use of anti-adhesive barriers and liquid media, as well as the use of modern compression hosiery for the prevention of thromboembolism and pulmonary embolism, can be considered a huge advantage for the prevention of the development of adhesive disease. After a year, as a rule, the site of the operation cannot be determined even with the help of ultrasound.
During laparoscopic nephrectomy
I make sure to remove all lymph nodes that may contain tumor cells. This step is extremely important, because it is impossible to exclude metastatic lesions of regional lymph nodes before surgery even using the most modern diagnostic method. If the lymph nodes affected by metastases are left, the process will progress. When mobilizing the kidney, modern ultrasonic surgical scissors are used, as well as an electrothermal dosed tissue ligation device “LigaSure” (USA) - thanks to which this stage of the operation is bloodless. The resected fragment with the tumor is removed from the peritoneal cavity in a special plastic container - this way contamination of the surrounding tissues with tumor cells can be avoided. At the same stage, an incision of about 4 cm is made on the abdominal wall.
I have extensive experience in minimally invasive surgical interventions; I have successfully performed about 500 operations for kidney tumors of various shapes - both benign and malignant. The results of the interventions are summarized in more than 20 scientific publications, which can be found in various peer-reviewed professional scientific publications, both in Russian and foreign.
I have been performing similar operations since 2000, during which time I have developed an original method of installing trocars during laparoscopic surgery on the kidney and retroperitoneum. This allows the instruments to be positioned at an optimal manipulation angle, so suturing the wound on the kidney during kidney resection and removal of lymph nodes during radical nephrectomy is easy and quick.
You can watch videos of operations performed by me on the website “Videos of operations by the best surgeons in the world.”
Patent for invention. A method for determining the optimal installation sites for manipulation trocars during laparoscopic operations on organs of the retroperitoneal space “Hand suture in endoscopic surgery”, K. V. Puchkov, D. S. Rodichenko
Knowing all the main methods of kidney surgery, having experience in successfully performing operations on cysts, benign tumors, as well as kidney cancer, I strive to select the optimal surgical treatment tactics in each specific case. The surgical techniques I use make it possible to perform operations using laparoscopic access that most surgeons perform only using open access, for example, during resection of a large cyst with a diameter of more than 10 cm or during nephrectomy for kidney cancer.
Today, my seminars on laparoscopic treatment of kidney tumors are attended by doctors - specialists from large scientific centers, hospitals of republican, regional or regional significance, as well as cadets of postgraduate education faculties.
For the development of methods of laparoscopic operations for the surgical treatment of kidney tumors, as well as other organs of the body, Professor Konstantin Viktorovich Puchkov was awarded one of the most prestigious awards in the field of surgery - “Golden Laparoscope”.
Kidney tumors
Kidney tumors account for 2-3% of all neoplasms. They are approximately 2 times more common in men than in women. Kidney cancer accounts for 5-6% of all urological diseases. The peak incidence occurs between 40 and 60 years of age. The incidence of kidney cancer increases from south to north and from east to west and in the Scandinavian countries and North America is 5-6 times higher than in Asia and Africa.
Risk factors for developing kidney cancer are excess body weight, smoking, long-term use of estrogens in men, contact with asbestos, employment in the tanning industry, and long-term hemodialysis.
Histologically, according to the classification of tumors and tumor-like formations of the kidneys, they are distinguished:
1. Epithelial tumors of the renal parenchyma:
- adenoma;
- cancer.
2. Epithelial tumors of the renal pelvis:
- transitional cell papilloma;
- transitional cell carcinoma;
- squamous cell carcinoma;
- adenocarcinoma.
3. Nephroblastic tumors:
- nephroblastoma;
- typical nephroblastoma;
- epithelial nephroblastoma;
- mesenchymal nephroblastoma;
- mesoblastic nephroma.
4. Nonepithelial tumors:
- benign (angiomyolipoma and others);
- malignant.
5. Mixed group:
- juxtaglomerular cell tumor;
- neuroblastoma and ganglioneuroma.
6. Secondary tumors.
7. Unclassified tumors.
8. Tumor-like processes:
- renal dysgenesis;
- vascular malformations;
- cysts;
- renal tubular hyperplasia;
- xanthogranulomatous pyelonephritis and malakoplakia;
- others.
Classification of kidney tumors according to the TMN system:
- T1 - the tumor is palpable, located in the center of the parenchyma, can only be detected by x-ray;
- T2 - the kidney with the tumor is palpable, but the tumor has not yet invaded the surrounding tissues;
- T3 - the tumor grows into the surrounding tissues, due to which the mobility of the organ is limited;
- T4 - the kidney and tumor are motionless, there are distant metastases.
The letter M denotes distant metastases to other organs, and N denotes metastases to regional lymph nodes. Metastases to regional lymph nodes do not occur at stage I of the process and not always at stage II. In stages III and IV, metastases in regional lymph nodes, as a rule, always occur.
Macroscopically, most often the kidney is tuberous due to protrusion of tumor-like nodes. On a section, the tumor has a variegated color (yellow-brown, red, gray, etc.). Histologically, kidney cancer consists of light brown, granular cell alveolar, fusiform, solid tubular, polygonal and other cells.
Malignant kidney tumors metastasize by hematogenous (through blood vessels) and lymphogenous routes. Metastases are observed in more than half of patients. The first place in the frequency of metastasis of kidney cancer is the lungs, then the bones, liver, and brain. This pattern is due to the presence of a close connection between the venous system of the kidney and the main vessels of the thoracic and abdominal cavities, as well as the venous network of the skeleton.
Often, kidney cancer metastases manifest clinically earlier than the primary site of the disease. A feature of kidney cancer is the relatively frequent appearance of metastases many years (10-15 and even 20) after removal of the primary tumor. At the same time, another feature of this type of cancer is that its pulmonary metastases in some cases tend to regress after removal of the primary lesion.
In second place in frequency among distant metastases of kidney tumors are bone metastases, which are most often localized in the pelvic bones, spine, ribs, bones of the shoulder girdle, femurs, and cranial vault. Metastases to the liver are observed in the later stages of the disease.
Regional metastases of kidney cancer mainly affect the paracaval and para-aortic lymph nodes.
In addition to distant and regional lymphatic metastases, kidney cancer metastasizes outside the lymph nodes into the perinephric fatty tissue, abdominal muscles, subcutaneous fatty tissue, and into the postoperative scar. In this case, it is not tumor germination that is noted, but the presence of separate, clearly demarcated foci of metastasis. In addition to metastasis of kidney cancer, tumor thrombus spread through the renal vein into the inferior vena cava is often observed.
The clinical manifestations of kidney cancer are very diverse.
There are renal and extrarenal symptoms. The classic triad of renal symptoms of kidney cancer - hematuria, palpable tumor and pain - occurs in 10% of patients and indicates an advanced process - about half of these patients have distant metastases at the time of diagnosis. One or two symptoms from the triad are more common.
One of the most common symptoms is hematuria, observed in 50-60% of patients, and in half of them this symptom is the first sign of the disease. Hematuria is always total, occurs suddenly, against the background of complete health, and is often not accompanied by pain. The occurrence of acute pain after intense hematuria is characteristic of tumor damage to the kidneys and is associated with obstruction of the ureter by blood clots. In non-tumor diseases also accompanied by hematuria (renal stones, hydronephrosis), pain usually precedes hematuria. Another characteristic feature of hematuria in kidney cancer is its intermittent nature with a tendency to shorten the intervals between repeated bleedings. There is no strict relationship between tumor size and the intensity of hematuria. A small tumor can be a source of massive hematuria.
The second most common symptom is pain in the lumbar region, occurring in 50% of patients. The nature of pain can be very diverse, and the occurrence of dull, intense pain of a radicular nature is an unfavorable prognostic sign.
A palpable tumor is detected in 30-40% of patients, and this symptom is rarely the only one and is usually combined with other complaints.
Of the extrarenal symptoms, fever is the most common, which in 4-6% of patients may be the only manifestation of the disease. Among the general symptoms of a kidney tumor, the deterioration of the general condition as a result of intoxication of the body with metabolic products in the tumor tissue is important. In this case, general weakness, loss of appetite, and weight loss are noted. Patients with such complaints are treated for a long time for a variety of suspected diseases before the idea arises of the need for a urological examination.
Weight loss as a manifestation of the tumor process is a consequence of the toxic effects of tumor decay products on the body. Intoxication leads to a decrease in appetite, which in turn causes weight loss. Weight loss is most often a sign of an advanced blastomatous process.
An important symptom of a general kidney tumor is an increase in body temperature. This symptom is observed in 20-30% of patients with kidney cancer. Sometimes an increase in body temperature is the only manifestation of the disease. Body temperature is often around 37 °C, but sometimes reaches 38-39 °C, accompanied by chills, simulating an acute infectious disease.
The toxic effect of a kidney tumor on the bone marrow leads to inhibition of its function and the occurrence of anemia, which is evidence of an advanced tumor process. The manifestation of a kidney tumor may be polycythemia or secondary erythrocytosis. This process is explained by increased production of erythropoietin by kidney tumor tissue. The most common general sign of a kidney tumor is an increase in ESR, which may be the first and only manifestation of the disease. In 5-10% of patients with malignant neoplasms of the kidney, the disease manifests itself as arterial hypertension.
An important local sign of a kidney tumor is a varicocele. Its causes in case of a malignant kidney tumor can be:
- compression of the left renal vein or its invasion by a tumor;
- bending of the left renal vein as a result of downward displacement of the kidney;
- compression of the inferior vena cava or directly one of the testicular veins by a tumor or packets of lymph nodes affected by metastases;
- thrombosis of the inferior vena cava.
Symptoms of kidney tumor metastases are varied. Metastases of kidney cancer to the lungs are often radiographically round in shape. Sometimes metastasis of kidney cancer to the lung, especially with a solitary tumor, progresses for a long time and is not clinically manifested. This situation is convenient for its prompt removal. The first clinical manifestation of kidney tumor metastases to the lung is hemoptysis. Metastases of a solitary tumor are often disguised radiographically as bronchogenic cancer, and multiple metastases may resemble the picture of pneumonia or pulmonary tuberculosis.
Metastases of a kidney tumor to the bone are clinically most often manifested by pain, often very intense and persistent, which does not subside even with narcotic drugs. Sometimes such pain is regarded as a symptom of radiculitis, intercostal neuralgia, etc. With metastasis to the spine, lower paraplegia and dysfunction of the pelvic organs may develop. The first symptom of the disease may be a pathological fracture at the site of metastasis. The most typical localization of bone metastases is the diaphyses of tubular bones (shoulder, femur), as well as flat bones - ribs, scapula, skull. A characteristic radiological sign of metastases of hypernephroid cancer in the bone is the osteolytic type of pathological process. Features of RP include the appearance in some cases of metastases many years after removal of the primary
Diagnostics. Upon examination and palpation, only advanced kidney tumors are usually detected. Upon examination, a varicocele can be detected, and with obstruction of the inferior vena cava, dilation of the veins of the anterior abdominal wall and swelling of the lower extremities.
Palpation of the kidney - the degree of mobility of the tumor or kidney during palpation to a certain extent serves as an indicator of operability.
Laboratory diagnostic methods include general blood and urine tests, biochemical and immunological studies. General blood tests reveal changes that are specific not only to kidney cancer: increased ESR, anemia. Urine tests reveal erythrocyturia. Proteinuria and leukocyturia may be observed, especially when a kidney tumor is combined with pyelonephritis.
Of the biochemical research methods, the most widely used are the study of enzymes, proteins and protein fractions, determination of calcium content in serum, and the Danilin reaction. Characteristic nonspecific signs for primary kidney cancer are increased activity of alkaline phosphatase and a number of other enzymes in the blood serum, increased levels of alpha2-globulin (Stauffer syndrome).
Recently, immunological methods have been used to diagnose kidney cancer. Using classical methods of immunodiffusion analysis (radial immunodiffusion reaction, immunoelectrophoresis, counter immunophoresis, double immunodiffusion according to Ouchterlony, etc.), it is possible to identify profound disorders in the metabolism of serum proteins; ferritin, transferrin, albumin, etc.
It has been established that kidney tumor tissue selectively accumulates ferritin. This protein is found in tumor tissue 10-220 times higher in concentration than in normal kidneys and cancerous tumors of other organs. The level of another iron-containing protein, transferrin, in the tumor tissue of the kidney is increased 3 times. These characteristic changes occur in the protein spectrum of the blood in 80% of patients. After nephrectomy, patients showed a tendency towards normalization of these indicators, which is evidence that the changes in serum proteins described above are pathognomonic for kidney cancer.
Taking into account the data obtained, it should be considered that an immunological examination if a kidney tumor is suspected should be a mandatory stage of a comprehensive examination of the patient.
In recent years, much attention has been paid to radioisotope diagnostics of kidney tumors. For this purpose, static nephroscintigraphy (or kidney scanning) is used.
Ultrasound scanning is widely used in oncourology for the diagnosis of tumors and kidney cysts. The method is harmless, safe, does not require preliminary preparation of the patient and has high diagnostic information content.
Ultrasonograms of a tumor are composed of pictures obtained after reflection of sound from dense inhomogeneous tumor tissues, blood vessels, hemorrhages, necrotic tissues, each of which has an acoustically demarcated surface. Thus, in the presence of a tumor, the contours of the kidney are deformed, and many echo signals appear inside the tumor due to uneven absorption of sound by the tumor. Ultrasound examination (ultrasound) can detect venous thrombosis, tumor ingrowth into blood vessels, and enlarged regional lymph nodes (LN), which makes it possible to determine adequate treatment tactics.
Ultrasound scanning of the kidney plays an important role in the differential diagnosis of a kidney tumor with pyonephrosis, hydronephrosis, polycystic kidney disease, and especially with a solitary kidney cyst. On scanograms, the cyst has a capsule with an even contour, inside of which there is a zone free from echo signals.
Despite the introduction of the above methods into clinical practice, the final stage in diagnosing a kidney tumor is an x-ray examination. Various x-ray methods are used to recognize the tumor process of the kidney.
An X-ray examination of the patient begins with a survey urography, which reveals changes in the configuration of the kidney and its position, and petrification in the tumor tissue. In some cases, when it is impossible to judge the contours of the kidney from a plain radiograph, they resort to tomography or pneumo-retroperitoneum, with the help of which a more relief image of the kidney shadow is obtained.
Excretory urography makes it possible to clarify both the functional and morphological features of the kidney affected by the tumor, and, in addition, to identify the condition of the opposite kidney. The function of the tumor-affected kidney in the initial stages of the disease remains quite satisfactory. The lack of function indicates an advanced blastomatous process, significant replacement of the kidney parenchyma with tumor tissue or infiltration of the renal pedicle or compression of it by packages of lymph nodes affected by metastases.
Abdominal aortography should be the first stage of renal angiography, at which the type of vascularization of the affected kidney is determined (single, double or accessory artery), the tumor is recognized, the nature of its growth (inward or outward), its relationship with surrounding organs, the presence of metastases in the opposite kidney , liver. Depending on the nature of vascularization, kidney tumors can be divided into two groups: avascular or hypovascular and hypervascular. The first group includes adenoma, adenocarcinoma, and kidney metastases. Hypervascular include most variants of renal cell carcinoma, which have a typical angiographic picture due to abundantly developed pathological vessels in the tumor.
Signs of a tumor are: expansion of the lumen of the main renal artery, disordered pathological vascularization in the tumor mass (a cobweb-like mesh in the tumor area and accumulation of radiopaque substance in the form of “lakes”, “puddles”, premature segmental nephrogram or image of the renal vein in the early arterial phase, increased shadow tumor mass, the presence of translucent lacunae and inhomogeneity of the shadow of the mass (tumor necrosis), etc.
Serial aortography is especially informative in this regard. The serial imaging program must be designed to obtain the early arterial phase to capture signs of fistula blood supply to the affected kidney.
Selective renal arteriography should be performed if it is necessary to clarify aortographic data.
If the presence of a tumor thrombus is suspected, inferior cavography and selective renal venography are the most informative.
Differential diagnosis
The greatest difficulties arise in the differential diagnosis of kidney cancer with small benign tumors, which make up 5-9% of all kidney tumors. Of the benign epithelial tumors, adenoma and oncocytoma are of greatest importance. Of the benign epithelial tumors of the kidney, adenoma is most often detected. This tumor is rare in people under 40 years of age and is observed in men 3-4 times more often than in women. A rare epithelial tumor of the kidney is
Kidney adenoma is represented by monomorphic cells with a correctly formed nucleus. The scanty cytoplasm of cells can be light or granular, or a combination of both mentioned characteristics. The tumor is delimited from the surrounding tissue, but is not surrounded by a capsule. Adenomas may be compact or contain cysts of varying sizes. Tumor cells form tubular or papillary structures. An adenoma is capable of invasive growth and metastasis, therefore it is proposed to regard a kidney adenoma larger than 2 cm as a malignant tumor and choose the appropriate treatment method.
Kidney adenomas usually do not appear clinically and are diagnosed accidentally. Ultrasound and computed tomography do not have reliable differential diagnostic features; with angiography, the tumor is most often avascular or hypovascular. Considering the difficulties of differential histological diagnosis of adenoma and cancer, renal adenomas larger than 3 cm of any degree of atypia are classified as cancer. In turn, adenomas include tumors of grade I atypia up to 3 cm in size.
Treatment: surgical
The term “oncocytoma” refers to a well-differentiated eosinophilic granular cell tumor of the renal parenchyma, consisting of oncocytes. In some cases, all cellular elements of the tumor or part of them have sharply eosinophilic fine-grained cytoplasm, rich in mitochondria, i.e. are so-called oncocytes.
A characteristic feature of oncocytes is their loss of organ-specific features. Tumors consisting of such cells can reach large sizes and appear as a node, clearly demarcated from the surrounding kidney tissue, with a brownish surface when cut, often with a scar in the center. In the differential diagnosis of oncocytoma, one should take into account the homogeneous appearance of the tumor, the absence of foci of necrosis and hemorrhages, as well as yellow areas characteristic of cancer.
The admixture of Sudan-positive cells in oncocytomas indicates the presence of fatty inclusions in the cells and indicates renal cell carcinoma. An important feature that allows differentiating oncocytoma from cancer is the absence of mitoses even with pronounced polymorphism of the tumor.
Clinical manifestations of oncocytoma occur when the tumor reaches a large size. Symptoms are more sparse than with renal cell carcinoma. In the angiographic diagnosis of oncocytoma, the “bicycle wheel with spokes” pattern, the absence of pathological vascularization, and the presence of a capsule or pseudocapsule are considered specific. In other cases, the picture of renal oncocytoma is indistinguishable from that of kidney cancer. The final understanding of renal oncocytoma has not yet been developed; treatment consists of kidney resection or nephrectomy, which is determined by the size and location of the tumor.
The next most common benign tumor is a mesenchymal tumor - angiomyolipoma. Its frequency is 0.3-5% of all kidney tumors, occurs 4 times more often in women than in men, and is diagnosed mainly at the age of 35-65 years. The tumor consists of tissues normally found in the kidney, but present in different proportions both in tissue structure and degree of maturity, and is therefore sometimes called a hamartoma. Angiomyolipoma is represented by fat cells, proliferations of smooth muscle cells and tortuous vessels, and their ratio can be different, to the point that in some cases the tumor in its composition is close to a single component - lipoma, leiomyoma or hemangioma.
Angiomyolipoma of the kidney occurs in 80% of patients with tuberous sclerosis (Bourneville disease), a congenital hereditary disease transmitted in an autosomal dominant manner. Such patients suffer from epilepsy and retarded mental development; they often have multiple tumors of organs of ectodermal origin (brain, retina, skin) and angiomyolipomas of organs of mesenchymal origin.
There are two clinical forms of the tumor. The first is often observed in combination with tuberous sclerosis, is detected at a young age, and is characterized by multiple bilateral lesions. The second form is detected in adulthood (40-60 years); Tumor nodes are usually unilateral and can reach large sizes. The ratio of men to women in any form is 1:4.
The clinical picture is dominated by pain, which is the result of hemorrhage into the tumor, which in some cases is accompanied by a picture of hypovolemic shock and acute abdomen. Gross hematuria is rare. Alternating multiple areas containing fat create a unique combination of hyperechogenicity on ultrasound and well-defined fatty inclusions on computed tomography, specific only to renal angiomyolipoma. A final opinion regarding treatment tactics has not been formed; tactics depend on the size of the tumor, clinical manifestations, and the presence of intercurrent diseases. For small asymptomatic angiomyolipomas, apparently, we can limit ourselves to observation. For large tumors, the treatment of choice is partial nephrectomy or nephrectomy.
In difficult diagnostic cases, percutaneous puncture biopsy of a renal tumor under the control of ultrasound or computed tomography is possible, which in 70% of cases makes it possible to make a morphological diagnosis.
Fibroids most often occur in the medulla of the kidneys. It is assumed that fibromas of this localization arise from the interstitial cells of the medulla and may have the ability to produce antihypertensive substances.
Hemangioma most often occurs in the wall of the renal pelvis, but can also occur in the area of the kidney pyramids. In a removed kidney, detection of hemangiomas is difficult due to the collapse of blood vessels.
Juxtaglomerular cell tumor consists of cells of the juxtaglomerular apparatus. This tumor is renin-secreting and consists of small cells that form fields and cords with perivascular orientation of cellular elements. The morphological determination of this type of tumor is based on the detection of renin secretion and diamond-shaped inclusions in the cytoplasm during electron microscopic examination.
In case of hydronephrosis, a tumor-like formation in the hypochondrium is palpated, but its consistency is tight-elastic, the surface is smooth, and hematuria is rarely observed. The pyelographic picture of hydronephrotic transformation differs sharply from the deformation of the pyelocaliceal system by the tumor. Renal arteriograms reveal narrowing of the lumen of the renal artery and its branches.
Polycystic kidney disease simulates a tumor in the case of its asymmetric development, when only one enlarged dense tuberous kidney is palpated. Suspicion of the presence of a tumor increases with hematuria. However, polycystic disease is characterized by chronic renal failure of one stage or another, and most importantly, a pathognomonic pyelographic pattern of bilateral changes, increased branching of the calyces, compression and elongation of the pelvis. On arteriograms, polycystic disease is characterized by the presence of many round avascular areas and elongated thinned arteries.
With a carbuncle (less often an abscess) of the kidney, suspicion of the presence of a tumor usually arises in connection with a similar x-ray picture (deformation, displacement of the pyelocaliceal system, amputation of the calyces). On scintiscanograms, the manifestations of the tumor and the renal carbuncle are also similar (focal defect in isotope accumulation). In addition, all clinical and laboratory signs of an acute inflammatory process (fever with chills, leukocytosis) not only do not exclude a kidney tumor, but are also quite characteristic of its symptoms. Renal arteriography brings clarity to the differential diagnosis in these cases.
Differential diagnosis of a tumor and kidney tuberculosis is carried out in a similar way.
Differential diagnosis of a kidney tumor and a retroperitoneal tumor can be very difficult. Palpation data for these diseases are the same. Using excretory urography and retrograde pyelography (preferably in combination with pneumoretroperitoneum and tomography), in case of a retroperitoneal tumor, displacement of the kidney is detected without deformation of the pyelocaliceal system and an image of a separately located tumor is obtained. Characteristic of a retroperitoneal tumor is deviation of the ureter in the medial direction.
Wilms tumor (nephroblastoma) accounts for 1/3 of all tumors in children and ranks first among all tumors in childhood. Children aged 2-5 years are most often affected. Girls and boys get sick equally often. Nephroblastoma is the result of a violation of kidney embryogenesis in the third period - the metanephros stage. In 1899, Wilsm indicated that these tumors were of mesodermal origin. According to his opinion, some mesoderm cells do not differentiate, but grow randomly and epithelial and connective tissue elements arise from them. Tumors range from 400 g to 12 or more kilograms.
Macroscopically, Wilms tumor consists of cavities with fluid or a gelatinous mass and dense tissue that looks like fish meat. Histologically, smooth and striated muscle fibers, cartilage, nerve formations, and epithelial cells can be identified.
Based on the degree of malignancy and histological structure, Hardwick and Stones distinguish 6 types of Wilms tumors. According to the degree of tumor spread and metastasis, 4 stages of the process are distinguished:
- Stage I - tumor in the capsule;
- Stage II - the tumor has grown into the capsule and there are metastases in the lymph nodes;
- Stage III - the tumor grows into neighboring organs;
- Stage IV - there are metastases to distant organs.
Early symptoms of Williams tumor include malaise, adynamia, irritability, capriciousness of the child, pallor of the skin, subfibrile temperature, periodic abdominal pain, traces of protein in the urine, and high ESR. These symptoms are not typical and do not always suggest a kidney tumor. Only the appearance of hematuria and the detection of a tumor in the abdominal cavity indicates kidney damage. It can compress the inferior vena cava or portal vein, which causes ascites or edema in the lower extremities. Hematuria occurs in 60-65% of cases, usually in the later stages of the process. A common symptom is hypertension, which is caused by compression of the renal parenchyma by a growing tumor.
Diagnosis of Wilms tumor is based on identifying clinical signs and carrying out special research methods: survey and excretory urography allows us to identify an enlarged shadow of the kidney and defects in the filling of the pelvis and calyces, their compression. The application of retropneumoperitoneum makes it possible to more clearly see the enlarged shadow of the kidney on x-ray and tomograms. Isotope scanning and renography reveal areas of decreased isotope accumulation and an incorrect type of renographic curve. In difficult and doubtful diagnostic cases, aortography and selective renal arteriography are performed.
Differential diagnosis of Wilms tumor is made with liver diseases, intestinal tumors, genital tumors in girls, Hirschsprung's disease and other diseases.
The best results are obtained by combined treatment (surgery, radiation and chemotherapy). Tumor removal in children is performed transperitoneally. Radiation therapy is successfully combined with the use of antitumor antibiotics (actnomycin D, chrysomalin, bruniomycin), which potentiate the effect of radiation. Among the cytostatics, vicristin, cyclophosphamide, etc. are widely used.
Prognostically, a 2-3-year survival rate is noted in 40-45% of those operated on.
Forecast. With a kidney tumor, the prognosis depends primarily on the stage of the process. The worst long-term treatment results were recorded in patients with renal vein invasion and metastases.
The prognosis is especially poor in non-operated patients. As the primary tumor grows or metastases spread, their condition steadily worsens: general weakness and exhaustion increase, in many cases fever, hematuria, and severe pain are noted. Patients die from severe intoxication, cachexia, and anemia.
An important prognostic factor is the age of patients; among patients under 40 years of age, lower survival rate was observed than among older ones.
Postoperative period
After the operation, 3-4 incisions remain on the skin of the abdomen, their length is no more than 5 mm, one incision is 4 cm, it is used to remove the removed organ. The patient can get up and take liquid food from the first day. The patient leaves the clinic on days 6-8. Working capacity is restored by 14-21 days after surgery. In the future, dynamic monitoring by an oncologist and urologist is recommended; an ultrasound scan must be performed 3 and 6 months after the operation.
Important! In the absence of metastasis in distant lymph nodes in patients with kidney cancer, radiotherapy and chemotherapy are not required. In the postoperative period, patients lead a normal lifestyle.
Questions most often asked by patients
— Is any preparation necessary for laparoscopic surgery for kidney cancer?
If you are planning surgical treatment for kidney cancer, I suggest you carefully study the section that is devoted to preoperative preparation.
— What type of anesthesia is used during laparoscopic surgery for kidney tumors?
In order to learn more about pain management methods during laparoscopic interventions for kidney tumors, you should carefully study the information posted on the website.
— Where can I undergo surgery for a kidney tumor?
I conduct initial consultations with patients with kidney tumors at the Swiss University Hospital. Check out the main clinical sites in Moscow and Switzerland.
Oncocytoma
Oncocytomas consist of large epithelial cells with eosinophilic granularity in the cytoplasm and are found not only in the kidney, but also in the adrenal gland, thyroid, salivary and parathyroid glands. Oncocytomas account for 3-5% of kidney tumors. Men get sick 2 times more often than women. The clinical course varies.
Macroscopically, oncocytoma is very different from kidney cancer. Oncocytoma, as a rule, has a clearly defined capsule, rarely invades the renal capsule, pyelocaliceal system and perinephric tissue, and has a bronze or light brown color on the section. In the center of the tumor, especially large ones, a stellate scar is often visible, but there is no necrosis typical of kidney cancer. Oncocytoma in most cases is solitary and unilateral.
Oncocytoma is usually detected by histological examination, since there are no characteristic clinical manifestations for this tumor. Gross hematuria and low back pain are observed in less than 20% of patients. CT, ultrasound, excretory urography and MRI also do not allow a diagnosis of oncocytoma. Angiographic signs such as the spoked wheel symptom (reflects the course of arterioles in the tumor), the presence of a transparent rim corresponding to the capsule, and uniform contrast in the nephrographic phase are not always observed in oncocytoma and occur in kidney cancer.
Foci of cancer may be detected in a well-differentiated oncocytoma. In addition, oncocytoma can accompany cancer of the ipsilateral or contralateral kidney. The risk of renal oncocytoma is increased in angiomyolipoma, tuberous sclerosis, multiple myeloma, lung cancer and carcinoids. Until recently, it was believed that well-differentiated oncocytoma is always a benign tumor. However, this opinion turned out to be erroneous, since several cases of the aggressive course of this tumor have been described.
Since it is impossible to diagnose oncocytoma before surgery, it is almost impossible to select patients with a well-differentiated tumor for organ-conserving surgery. The role of cytological examination in the diagnosis of oncocytoma is controversial. Nevertheless, the characteristic cytological signs of oncocytoma have already been described, and some authors recommend determining the indications for organ-preserving surgery based on the results of a cytological study.