Neuropsychology is a branch of psychology devoted to the study of the brain mechanisms of higher mental functions based on observations of local brain lesions. The foundations of Russian neuropsychology were laid by A.R. Luria, who developed the theory of systemic dynamic localization of mental processes. The leading research method in neuropsychology is syndromic analysis of disorders of higher mental functions, which provides a qualitative qualification of these disorders and a topical diagnosis of brain damage.
Neuropsychology
Neuropsychology is a clinical and experimental discipline concerned with the study, explanation, assessment and management of behaviors directly related to the functioning of the brain. Although neuropsychology primarily deals with people with brain lesions, the discipline also examines individual differences between people with normal brains due to differences in its structural and functional organization. Neuropsychology is a field formed by the branches of psychology and neuroscience, and as such is closely related to behavioral neuroscience. Many people working in this field, instead of basic training in psychology, receive the specialty of neurologist while studying at medical institutes.
Historical development
The connection between brain functioning and behavior has been documented since 3500 BC. e. in the papyrus of Edwin Smith, and there is some reason to believe that this connection was noticed back in the Upper Paleolithic era. Since time immemorial, theorists have agreed that the thinking and intellectual abilities of people. associated with the brain, but there was fundamental disagreement among them about which brain structures are responsible for intelligence. Modern Concepts of brain functioning began to develop only in the 19th century.
Gall was the first major researcher to suggest that specific psychol. functions are localized in specific organs or areas of the brain, a theory believed by the French surgeon P. Broca. Based on the results of autopsies of two patients who had lost the ability to use expressive speech, Broca reported that he had discovered a zone of the brain in which the motor center of speech is localized. Considered by many as a major achievement, Broca's work sparked an endless stream of research efforts to establish the brain localization of specific psychol. functions.
Despite the fact that localization theories were especially popular in the 19th century, many scientists rejected them. Flourens launched a series of attacks in defense of the theory of equipotentiality, according to which intellectual and psychological skills are a product of the activity of the brain as a whole, and not of its specific individual parts. At the beginning of the 20th century. many neuroscientists have adopted the equipotential approach. Although these theorists agreed that the main motor and sensory functions are localized in certain areas of the brain; higher intellectual functions, in their opinion, are the result of the functioning of the entire brain. Any brain lesion, regardless of location, will impair these higher intellectual skills.
Both theories have had a significant impact on the assessment of brain damage in clinical neuropsychology. Experts advocating equipotential view have focused on the search for a test or tests that could measure the basic higher intellectual skills that suffer in all forms of brain damage. Psychologists who take the position of localization have focused on searching for tests that measure each psychol. a skill mediated by the brain, allowing it to evaluate not only psychol. skills directly related to the brain, but also their localization in specific brain areas.
What is neuropsychology
Take the survey and find out how neuropsychology can help you
If you answered “Yes” to at least one question, then neuropsychology is definitely right for you
What is neuropsychology? This is a modern scientific direction, formed in the mid-20th century, which studies the connection between brain functions and mental processes, making it possible to determine the influence of different parts of the brain on the personality, behavior and development of living beings.
Any mental or physical activity is a complexly organized system of signals and impulses in the brain. Mastering any skill requires the coordinated work of all parts of the brain throughout life.
Content
The main tasks of neuropsychology.
1) The relationship between the work of certain parts of the brain in contact with the outside world. 2) Identification of patterns of changes in brain organization during local brain damage. 3) Assessment of the performance of the brain as a whole and its individual structures. 4) Early diagnosis of syndromes of focal brain lesions on the border between health and disease.
Areas of neuropsychology.
In neuropsychology, there are several areas that differ in their tasks. The main ones are clinical, rehabilitation and experimental.
Clinical is a branch of neuropsychology specializing in the study of patients with lesions in various parts of the brain. This is of great practical importance, as it helps to predict, diagnose and treat patients. The main method of treatment is a neuropsychological examination, proposed by the scientist A. R. Luria.
Rehabilitation – deals with the restoration of higher psychological functions in case of partial brain damage, as well as the restructuring of impaired functions for the subsequent possible interaction of the patient with the everyday and social spheres. The main method of treatment is a set of techniques that influence weakened functional parts of the brain.
Experimental – studies processes associated with local brain lesions. Most often it is memory and speech. The main treatment method is electric shock. There are no clear boundaries between these directions. These methods are aimed at studying memory, speech, thinking and writing. Recently, neuropsychology of childhood and later life has also been identified as separate areas. The main objectives are to study ontogenetic features in the process of maturation of the cerebral hemispheres and age-related changes in the central nervous system.
Who is a neuropsychologist?
A neuropsychologist or a clinical psychologist (these are different things. Although a neuropsychologist is nowhere without knowledge of clinical psychology. Still, these are different specifics of work. Clinical psychology is closer to medicine) is a specialist whose work is based on knowledge of the laws of the human nervous system and his task is to correct undeveloped mental functions. This specialty is not related to medicine and consists of correct and competent consultations with clients who have suffered as a result of the disease. His responsibilities include studying the individual characteristics of the patient and adapting to everyday and social conditions. (adaptation to everyday and social conditions is carried out by a defectologist. Neuropsychology is, after all, work with those who have a cortex. It is diagnosis, correction and rehabilitation. Ideally, this is work with normotypical children with developmental disabilities)
In modern society, in most cases, clinical psychologists work with children suffering from developmental delays. Neuropsychological care for adults is also relevant, but less known.
When to contact a pediatric neuropsychologist?
− the child lags behind his peers in development; − when doing school homework, the child gets tired quickly, remembers poorly, and attention is distracted; − the child has low motivation to learn; − uncertain and awkward movements of the hands; − speech development disorders; − emotionality and increased activity in movement; − risk of hereditary disease.
What is neuropsychology? This is a way to help yourself. A person can visit this specialist after experiencing stress, illness and nervous overload, as well as for his own effectiveness (the ability to correctly express thoughts and develop memory).
Psychological Training Center Orange Sun
The role of neuropsychologists
Since the 1960s. neuropsychology began to evolve into an increasingly specialized field, staffed by people with training beyond the scope typically received by clinical psychologists. Once involved only in identifying patients with local brain damage among other categories of patients, psychologists are now involved in accurately determining the nature and extent of brain damage, evaluating therapeutic programs, predicting treatment outcome, and planning rehabilitation programs.
New fluoroscopy techniques make it possible to detect atrophy of brain tissue without pain or significant harm to the patient’s life. Therefore, many diagnostic services previously requested from psychologists have become the responsibility of a neurodiagnostician. And this, as many have argued, suggests that the psychologist should play a different role in neurodiagnostics.
One alternative role involves conducting a thorough analysis of the brain syndrome as it is expressed in a particular patient. This assessment includes assessment of qualities such as general intelligence, perceptual-motor functioning, speech, flexibility, reaction speed, attention and concentration.
Main directions of scientific research in neuropsychology
– Cultural-historical concept of mental development, participated in the creation of the theory of activity. On this basis, he developed the idea of the systemic structure of higher mental functions, their variability, plasticity, emphasizing the lifetime nature of their formation, their implementation in various types of activities.
– Investigated the relationship between heredity and upbringing in mental development. Using the twin method traditionally used for this purpose, he made significant changes to it, conducting an experimental genetic study of the development of children in conditions of the targeted formation of mental functions in one of the twins. Showed that somatic symptoms are largely determined genetically, elementary mental functions (for example, visual memory) - to a lesser extent. And for the formation of higher mental processes (conceptual thinking, meaningful perception, etc.), the conditions of education are decisive.
– In the field of defectology, he developed objective methods for studying abnormal children. The results of a comprehensive clinical and physiological study of children with various forms of mental retardation served as the basis for their classification, which is important for pedagogical and medical practice.
– Created a new direction - neuropsychology, which has now become a special branch of psychological science and has received international recognition. The development of neuropsychology began with studies of brain mechanisms in patients with local brain damage as a result of injury.
– Developed a theory of localization of higher mental functions,
– formulated the basic principles of dynamic localization of mental processes,
– created a classification of aphasic disorders and described previously unknown forms of speech disorders,
– studied the role of the frontal lobes of the brain in the regulation of mental processes,
– studied the brain mechanisms of memory.
Areas of neuropsychology
Acceptance of this new role has raised important questions regarding the relationship of neuropsychology to traditional models of professional training in psychology. Some neuropsychologists are beginning to consider themselves to be a separate subspecialty, similar to how clinical psychology is recognized as a subspecialty. In contrast, others perceive neuropsychology (especially its branches dealing with assessment and treatment) as a subspecialty of clinical psychology. In this model, training in clinical psychology is complemented by specialization in N.
Neuropsychologists with different orientations may also view patient populations and practice very differently. Psychologists trained in the neurological tradition most often see patients with obvious deficits in brain function, especially patients suffering from aphasia, due to the importance that many prominent neurologists attach to speech disorders. The examination methods they use are predominantly qualitative, focused on identifying how the patient performs a particular task, and not on using indicators obtained from more traditional psychol. tests. Testing procedures may be standardized, but they are often modified to suit the perceived needs of the individual patient and the impressions of the examiner.
In contrast, other psychologists may take a more quantitative approach to these problems, borrowing from the rich tradition of quantitative psychometric assessment. There are different variations of this approach, with some, such as the use of a single test, falling into obscurity, while others, such as the use of batteries of tests, are gaining increasing popularity. In any case, the quantitative approach emphasizes establishing norms for test scores and justifying the ability to objectively analyze the patient's demonstrated deficits rather than relying on purely intuitive assessment. However, the effectiveness of this approach still depends on the knowledge and experience of the clinician, since test performance patterns can change under the influence of a large number of variables, including the area of local brain damage, the speed of the pathological process, the nature of the damage, premorbid intellectual level, the degree of functional recovery, and many others.
Conceptual apparatus of neuropsychology
In the conceptual apparatus of neuropsychology, two classes of concepts are distinguished:
- a class of concepts common to neuropsychology and general psychology;
- a class of neuropsychological concepts proper.
Concepts such as higher mental function, mental activity, mental process, personal meaning, image, sign, action, operation, meaning, internalization and many others relate simultaneously to neuropsychology and general psychology.
The second class includes concepts that reflect the application of general psychological theory to neuropsychology.
Both general psychology and neuropsychology understand higher mental functions as complex forms of conscious mental activity. They are based on appropriate motives, which are regulated by certain goals and programs and are subject to the laws of mental activity.
Higher mental functions are formed under the influence of social factors during life; they are mediated in their psychological structure and arbitrary in their method of implementation.
As systems, higher mental functions are plastic, and their components are interchangeable.
The actual neuropsychological concepts include:
- primary neuropsychological symptoms;
- norm of function;
- secondary symptoms;
- neuropsychological syndrome;
- neuropsychological factor;
- neuropsychological symptom;
- neuropsychological diagnostics;
- syndrome analysis;
- functional system;
- brain mechanisms of higher mental function;
- localization of higher mental function;
- interhemispheric interaction, etc.
Mental function can be impaired as a result of local brain damage, which is a neuropsychological symptom, and their combination represents a neuropsychological syndrome caused by damage to a certain factor.
The neuropsychological factor is a structural and functional unit of the brain with a certain principle of physiological activity - when this activity is disrupted, a neuropsychological syndrome appears.
To discover a common factor that explains the origin of neuropsychological symptoms, they resort to syndromic analysis.
There are special clinical neuropsychological methods that help examine patients with local brain lesions - this is neuropsychological diagnostics, the purpose of which is to establish the location of the brain lesion.
The neuropsychological diagnosis of disorders of higher mental functions is based on the norm of function.
The normal function is characterized by variations depending on gender, age, type of hemispheric organization of the brain, etc.
Note 1
There are much more concepts related to the actual neuropsychological ones, and they all relate to the basic conceptual apparatus of the theory of systemic dynamic localization of higher mental functions of a person.
Controversial issues in neurodiagnostic testing
There are a number of important debates in neuropsychology regarding the choice between individual and standardized testing, quantitative and qualitative testing, single-dimensional (using a single test) and multi-dimensional (using test batteries) testing, as well as the role of the clinical psychologist and rehabilitation programs.
Individual versus Standardized Testing
Proponents of an individualized approach usually advocate the choice of tests for a patient based on medical results. examination, anamnesis and clinical picture at the initial and subsequent stages of treatment. Neuropsychologists who use this approach argue that individualized assessment allows the clinician to concentrate testing efforts on those areas where a given patient shows the greatest deficits. In theory, this approach allows the clinician to conduct a thorough assessment of the patient in a shorter time. Opponents of this approach note that the accuracy of individualized assessment depends largely on the skill of the individual clinician. When the clinician's subjective judgment informs the selection of appropriate tests, such testing can be highly effective. If, however, the tests selected do not adequately measure the patient's functional deficits, the individualized assessment may be insufficient at best or misleading at worst. Moreover, opponents argue, this approach does not allow for the collection of systematic data by either category of patients or categories of disorders; as a consequence, the possibilities for drawing conclusions from the results of an examination of a group of patients, or at least for scientific confirmation of the reliability of such conclusions, are significantly limited.
Because of these limitations, many clinicians use standardized tests or test batteries tailored to what they believe to be essential. measurements relevant to the assessment of suspected brain dysfunction. All patients are assessed on these measurements. Of course, the standardized approach has its limitations. First of all, the more parties involved in the survey, the longer it takes; The most complete comprehensive battery of tests may require a full day or more to complete. In addition, tests included in standardized batteries addressed to all patients in general may sometimes not be suitable for assessing areas that are relevant to that particular patient.
An effective compromise solution to overcome the limitations of standardized testing is to combine this approach with more flexible additional testing.
Quantitative/Qualitative Testing
The quantitative approach involves reducing all the features of the test to a set of numbers, which can be used to compare the patient’s results on this test with the results obtained in normative groups of healthy people and patients with brain lesions. Based on such comparisons, a diagnostic decision can be made. Proponents of the quantitative approach emphasize its reliance on objective indicators, which are characterized by reproducibility across a variety of researchers and clinicians, and its emphasis on scientific research. results obtained under controlled conditions.
The qualitative approach emphasizes how a particular person. tries to complete the test, and not the number of points he scored. This gives the clinician the opportunity to understand the important underlying processes that determine the quality of the patient's test performance. Once these underlying processes are understood by the clinician, the clinician can identify the cause of brain dysfunction and assess its implications for the patient's recovery and rehabilitation.
These approaches should not be viewed as mutually exclusive. Effective clinicians often combine both approaches.
Single tests/test batteries
Traditionally, many psychologists have used only one test to assess disorders associated with localized brain lesions. However, it is now recognized that the single test approach to assessment is generally ineffective. Therefore, many clinicians have adopted a multitest approach, in which diagnostic decisions are made based on the patient's cumulative test performance. Ideally, the tests included in the battery should represent the different abilities affected by brain lesions.
The use of test batteries also leaves more room for complex interpretative approaches. The results of a test designed for right-hemisphere performance can be compared with the results of a test designed for left-hemisphere performance. Verbal tests and tests of right-sided motor and sensory functions are considered to reflect left-hemisphere performance, whereas nonverbal tests and tests of left-sided motor and sensory functions are considered to reflect right-hemisphere performance.
When working with test batteries, configuration analysis can also be used. Configuration analysis is probably one of the most powerful tools available to clinical neuropsychologists to analyze more difficult, subtle cases of organic brain syndrome.
A wide variety of tests are used in neuropsychological assessment, both individually and as test batteries. Among the individual tests, some of which are presented as part of others, we can name the Bender Gestalt Test, Memory for Designs, Token Test, Benton Visual Retention Test, subtests from the Wechsler Adult Intelligence Scale, Boston Boston Diagnostic Aphasia Examination, Perdue Pegboard, Stroop Color and Word Test, and Wisconsin Card Sort Test.
In addition, there are a number of test batteries, but most are used in only one or a relatively small number of contexts. Two batteries, the Halsted-Reitan Neuropsychological Battery and the Luria-Nebraska Neuropsychological Battery, have received the most widespread attention. The Halsted-Reitan battery predates the Luria-Nebraska battery and has been in use since the 1950s. Perhaps this battery, more than anything else, is responsible for the increased popularity of clinical N.
The Luria-Nebraska Neuropsychological Battery is a newer test, introduced in 1978. This battery was a departure from standard tests in that it combined Luria's qualitative, behavioral, neurological approach with Reitan's standardized, quantitative approach. This test emerged as a unique approach for neuropsychological assessment and has therefore generated heated and widespread controversy. Despite the heated debate surrounding its use, it has become one of the main ones. tests used in the field and is now taught in an increasing number of programs. The interpretation is made on the basis of an analysis of the configurations, supplemented by observations of how the patient performed the tasks included in the battery. These qualitative observations are now organized in a form that allows frequency analysis, etc. so are formalized. The strength of the Luria-Nebraska Battery lies in the integration of qualitative and quantitative approaches and the greater research opportunities provided by the quantitative system.
NEUROPSYCHOLOGY
NEUROPSYCHOLOGY (from neuro... and psychology), a branch of psychology aimed at studying the brain mechanisms of mental health. processes. N. developed at the intersection of psychology, neurology, and physiology and is one of the areas of modern science. neuroscience. The term "N." first appeared in the work of D. O. Hebb (“The organization of behavior: a neuropsychological theory”, 1949) and became widespread in the 2nd half. 20th century
N.'s history is connected with the confrontation between two main principles. approaches to solving the problem of mental localization. functions. The discovery of the motor center of speech in 1861 by P. P. Broca (in the posterior part of the third frontal gyrus of the cortex of the left hemisphere) and the subsequent discovery in 1874 by K. Wernicke of the sensory center of speech (in the posterior part of the first and second temporal gyri of the cortex of the left hemisphere) became the basis of narrow localizationism , based on the idea of the brain as a collection of organs, each of which is associated with a specific mental. function (F. J. Gall, Broca, Wernicke, K. Kleist, etc.). Proponents of anti-localizationism - functional equipotentiality (P. J. M. Flourens, K. S. Lashley, etc.), starting from the plasticity of the brain, its ability to compensate for possible damage, sought to prove that any mental. the function is ensured by the work of the entire brain. Eclectic attempts have been made. combining these theories: if elementary functions can be localized, then higher ones are provided by the work of the entire brain (K. Goldstein, G. Head, etc.).
A. R. Luria developed the theory of system dynamics. localization of higher mental functions of a person (its creation was significantly influenced by the works of L. S. Vygotsky and P. K. Anokhin), in which complex forms of mental. activities are considered as functional systems ensured by the work of the entire brain; Moreover, each part of the brain contributes specifically. contribution to the construction of these systems.
Luria identified three functional blocks of the brain, defining the specialization of each of them in providing complex forms of mental health. activities. The brain stem and reticular formation provide energy. cortical tone and are involved in maintaining wakefulness. The temporal, parietal and occipital regions of the cerebral cortex are an apparatus that ensures the receipt, processing and storage of modality-specific (auditory, tactile, visual) information that enters the primary sections of each cortical zone, is processed in more complex secondary sections of these zones and is combined, synthesized in tertiary zones (or “overlap zones”), especially developed in humans. The frontal, premotor and motor areas of the cortex are an apparatus that ensures the formation of complex intentions, plans and programs of activity, implementing them in the system of corresponding movements and making it possible to exercise constant control over their course.
To identify the role of specific areas of the brain in providing mental health. qualities and properties that act as links in the structure of decomposition. psychic functions, A. R. Luria developed a neuropsychological procedure. syndromic analysis, which makes it possible to identify a complex of higher mental disorders during examination of patients with focal brain lesions. functions and their connection with the affected area of the brain.
Until 1970 divers. aspects of N. were associated with the description of neuropsychological. syndromes and formulation of topical diagnosis. This situation changed with the introduction of modern neuroimaging methods, first with computed tomography (1973), then in the 1980s. functional magnetic resonance imaging and positron emission tomography. Clinical N. focused on creating functional descriptions of mental defects. processes that are important in determining treatment and rehabilitation strategies. In experimental N. it means. place was taken by comparison of neuropsychological. mental models functions with data obtained by functional neuroimaging methods. Dr. directions N.: rehabilitation, psychophysiological, cognitive, individual differences, childhood and age of involution.
Rehabilitation
Area of planning and implementation of rehabilitation programs, main. according to neuropsychological data, is still in an “infantile” state. Systematic scientific research. little work has been done in this area, despite growing interest in patients with cerebrovascular disorders and head injuries. Much more has been done for people with peripheral disabilities. The work of scientists such as Diller, Ben-Ishei, Gertsman, Goodkin, Gordon and Weinberger indicates the potential high level of assistance that can be offered using cognitive remediation training techniques even to people with relatively severe disorders.
Theoretical positions
There are leading theoretical schools in neuropsychology. The core of these leading schools of neuropsychological thought is the localizationist and equipotentialist theoretical positions.
Equipotential theory
Equipotential theory, as mentioned, is associated with the assumption that all brain regions contribute equally to overall intellectual function. Thus, the specific area of brain damage is not important, and only the degree of its damage determines behavioral deficits. Many representatives of the equipotential approach emphasize deficits in abstract or symbolic abilities, which presumably accompany all forms of brain damage.
Equipotential theory had a strong influence on the development. psychol. tests. Although tests had already been developed on which individuals with brain lesions scored consistently lower than those without such lesions, these tests did not have sufficient discriminative power to be used in current clinical work.
Localization theory
Localization theory suggests that each area of the brain is responsible for specific psychol. skills. Therefore, the main concern in assessing organic brain lesions is to find out where in a particular person. the lesion is localized. The extent of damage is only important insofar as more extensive damage affects more areas of the brain and therefore impairs more skills. But lesions of approximately the same size in different parts of the brain cause significantly different effects. When assessing a particular patient, a psychologist working within this theory is forced to recognize that very few lesions are truly limited to a specific area. Tumors, for example, can cause increased intracranial pressure, thus affecting. areas of the brain located at a considerable distance from the tumor itself. Head injuries disrupt the functions of not only the hemisphere that was directly affected by the blow, but also the functions of the opposite hemisphere, which, due to displacement, received an indirect blow from a collision with the bones of the skull. Stroke victims often exhibit poor cerebral circulation in general. With almost any brain injury, many skills associated with areas distant from the lesion are impaired, especially in the acute phase of the disorder.
Alternatives
Neither the equipotential theory nor the localization theory receives complete confirmation in psychology. research The equipotential theory cannot explain the specific, limited deficits that arise in certain patients without k.-l. general deterioration of abstract abilities or other similar skills. Localization theories have serious difficulty explaining why a specific deficit such as dysgraphia can appear in almost all focal lesions of the left hemisphere and in many lesions of the right hemisphere.
With no basis to definitively accept one of these two theories, many have turned to searching for an alternative. The creation of one such model is credited to J. H. Jackson, an English neurologist. Jackson noticed that most psychol. functions are not unitary abilities, but are collected from more elementary skills. According to Jackson, even though these elementary skills themselves may be localized, all observable behavior is a complex interaction of multiple elementary skills, and therefore most actual behavior involves the brain as a whole. Thus, his theory combines localizationist and equipotential views, acquiring the ability to explain experiments. data collected in support of both viewpoints.
Jackson's views received the greatest development in the theories of the Russian neuropsychologist A. R. Luria. In Luria’s view, all behavior is fundamental. on functional systems, and specific patterns of interaction between local brain regions are required to give rise to specific behavior. Any damage to the brain that destroys any part of the functional system will lead to disruption of all forms of behavior, mainly. on this system. Consequently, the most complex intellectual skills, such as abstraction, will be the most susceptible to brain damage, since a large variety of functional systems must be involved in the production of such behavior.
Neuropsychology and brain disciplines
What does neuropsychology study?
- Neuropsychology studies the psychological structure, brain organization of: non-speech HMF (various types of non-speech gnosis and praxis); speech function.
- Disorders of speech and other HMFs, their diagnosis and methods of correction and rehabilitation work in the development process; during maturity
- Disturbances of speech and other HMF depending on brain damage - local, diffuse, interzonal connections of the conductor - nerve pathways).
Implications for other disciplines
- For neurology and psychiatry:
Neuropsychology allows you to take into account:
– state of the HMF for diagnosis and treatment of patients;
– features of interaction between the cerebral cortex and deep structures;
– features of consciousness, thinking and memory from the point of view of their brain mechanisms
- For defectology:
Neuropsychology allows
– understand the brain mechanisms of various developmental disorders;
– expand the range of diagnostic methods;
– analyze the structure of the defect in the affected function (identifying primary and secondary symptoms) to understand compensatory changes and select methods of targeted influence;
– choose the optimal methods of correctional work based on the patterns of interzonal interactions in the brain.
- For psychiatry:
Neuropsychology allows you to:
– carry out differential diagnosis of behavioral disorders caused by changes in consciousness during mental illness and loss of the ability to use language to express thoughts;
– optimize treatment methods in accordance with the results of neuropsychological diagnostics, identifying the primarily affected levels and areas of the brain.
E.D. Chomskaya, a long-time colleague of A.R. Luria, in the textbook “Neuropsychology” she created in 1987, various sections of this discipline are highlighted.
The main one is clinical neuropsychology, the task of which is to study neuropsychological syndromes, understood as a set of symptoms caused by a particular lesion.
The importance of a qualitative analysis of syndromes, their comparison and determination of the topic (localization) of the lesion is pointed out. For this, clinical neuropsychology has its own tools - specific diagnostic methods.
Some of them were proposed by the classics of neurology of the past, but in general the diagnostic neuropsychological system was created by A.R. Luria. It has become widespread not only in our country, but also abroad.
Another branch of neuropsychology is experimental neuropsychology. It is aimed at studying various forms of HMF disorders.
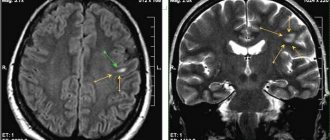
Within its framework, both neuropsychological diagnostic methods and instrumental ones are used, which have recently become very diverse and informative: EEG - electroencephalographic studies; CT - computed tomography; NMR - nuclear magnetic resonance; MRI - magnetic resonance imaging; PET - positron emission tomography; SPECT - single-phase positron computed tomography, etc.
As a result of experimental neuropsychological studies, the brain mechanisms of various types of agnosia and apraxia, speech disorders, memory, attention, regulatory (frontal) mechanisms of the psyche have been described, classifications of forms of aphasia have been created, the most common of which is the classification of A.R. Luria.
Within the framework of neuropsychology, there is also a section of neurorehabilitation. The main developments in this area are being carried out at the Moscow Center for Speech Pathology and Neurorehabilitation under the scientific supervision of Professor, full member of the Academy of Russian Academy of Education V.M. Shklovsky.
The main task of neurorehabilitation is the development of methods for restoring impaired HMF, differentiated in relation to the acute and residual (remote) stages of the disease.
The combination of methods used constitutes a comprehensive system of neurorehabilitation aimed at restoring the motor and analytical spheres, speech and other types of higher mental activity, as well as the social status of the patient.
The problem of adaptation of a person who has lost such important functions as movement, memory, speech, i.e. his adaptation to changed living conditions covers relationships with family members (intrafamily), as well as with strangers (extrafamily).
This means that neurorehabilitation includes not only the treatment and rehabilitation direction itself, but also one that provides ways to improve the future fate of the patient: professional diagnostics and vocational guidance.
Identifying the real abilities for certain types of labor and social activities of people whose vital functions have been affected makes it possible to determine the optimal type of employment available to them.
Otherwise, the life of healthy family members is disorganized, which leads to significant losses on a public and national scale.
Relatively recently (in the 70s), a section of neuropsychology emerged, designated as childhood neuropsychology or, in other words, developmental neuropsychology or developmental neuropsychology. A significant contribution to this area in the 80s of the last century was made by A.R. Luria’s student E.G. Simernitskaya.
Developments by E.G. Simernitskaya and subsequent researchers showed that for children under 10 years of age, unlike adults, lesions in the right hemisphere of the brain are extremely significant.
Did not you find what you were looking for?
Teachers rush to help
Diploma
Tests
Coursework
Abstracts
They lead to disorders of those HMFs, including speech, which in adults are upset in most cases when the left one is affected. Based on the observation, a fundamentally important conclusion was made that in children the brain organization of the HMF is different than in adults.
The peculiarity of HMFs and their brain organization is that they change from age to age. They receive a more specific and stable representation in one or another part of the brain, as a result of which their connections with other areas become less mobile.
This, on the one hand, facilitates the diagnosis of disorders, and on the other hand, deprives children of one of the main advantages - brain plasticity, which provides high compensatory potential.
Neuropsychological studies conducted on children have made it possible to determine the chronological (temporal) sequence of maturation of HMF.
Thanks to this, parents, doctors, and teachers can monitor whether the child is developing correctly, so as not to miss time in acquiring the necessary skills, which in the future may become irreplaceable. L.S. wrote about the extreme importance of this information. Vygotsky
Finally, there is the neuropsychology of old age, which has not yet been developed much, but is very relevant for understanding the nature and treatment of various senile degenerations, including dementia.
It should be added to the above that the neuropsychological method turns out to be fruitful for solving general problems of psychodiagnostics. WITH
This includes, first of all, the problems of individual differences in the study of human personality: determining the quality and degree of giftedness of children and adults, the behavior of people placed in extreme situations, etc.
In the development of these branches of neuropsychology, a special role is played by ideas about the meaning of individual, naturally determined relationships that develop between the hemispheres of the brain.
Individual differences in the volume and activity of interanalyzer connections are also significant. They are caused by innate “accents” on one or another analyzer, according to which people are divided into predominantly “listening”, “looking”, “sensing”, “smelling”.
Individual preference for auditory or visual types of perception and memorization of reality phenomena is especially relevant. It was found that in some types of activity, for example, in speech, the auditory analyzer dominates (dominates) in all people, and in others, for example, in the knowledge of the objective world, the visual analyzer dominates.
These analyzers are closely interconnected, their work is friendly. As it turned out, motor and tactile reinforcements are also important for analyzer interactions.
For a number of people, they are a necessary condition for the development of certain skills, even of higher mental activity (counting, tapping, speaking, etc.).
Understanding this has led to the creation of an arsenal of audiovisual and kinetic teaching methods that have proven themselves in various fields of pedagogy, psychology, psychotherapy, etc.
The extent of participation of one or another type of perception varies individually. This, unfortunately, is not always taken into account in schools, where the pace of children’s activities is averaged, namely, looking around, listening to something, reading, and writing arithmetic.
This often leads to difficulties in learning the necessary information and, ultimately, to a decrease in academic performance. Neuropsychological methods for diagnosing and monitoring the dynamics of the results of the educational process at school are very useful, although they are not yet used enough in practice.
Neuropsychology has its own methodology for considering certain pathological phenomena, its own terminology and conceptual apparatus. Some of the terms and concepts used in it coincide with those used in other disciplines, and some are specific to neuropsychology.
Thus, the concepts and terms of etiology, clinical picture, and pathogenesis are universal. They mean the same thing in both medicine and neuropsychology. Etiology is the cause or origin of a phenomenon, in particular a disease or disorder.
The clinic is a picture of a pathological condition, a set of symptoms that define it. Pathogenesis is those natural or individual reactions with which the body responds to pathological influences. In neuropsychology, this is primarily an effect on the brain.
They are mechanisms for the development of a disease or disorder. Pathogenetic mechanisms determine what form a particular disease takes and its consequences.
There are also concepts and terms that are used primarily in neuropsychology, even if they originated within other disciplines.
These include the concepts of gnosis and agnosia, praxis and apraxia, modality, modality-specific and modality-nonspecific phenomena, the concepts of kinetic and kinesthetic, afferent and efferent signals, etc.
A.R. Luria introduced into neuropsychology the extremely important concept of factor analysis, which reveals the meaning of primary and secondary symptoms, as well as the features of their relationship for the characteristics of the syndrome, which is a set of symptoms as a whole.
Primary symptoms are those that are caused directly by the lesion or other damage to the brain, and secondary symptoms are those that occur systemically, i.e. follow from the primary ones and are their consequence.
For example, a patient has articulation defects, despite the fact that there is no lesion in the area where articulatory postures and movements are localized.
In this case, they may be a systemic consequence of another defect, namely the vagueness of acoustic ideas about the pronounced sounds of speech, caused by damage not to the articulatory, but to the auditory cortex of the brain.
Correctly conducted factor analysis makes it possible to determine the strategy and tactics of correctional and restoration work in each specific case.
The recognition of natural systemic symptoms in a particular pathological syndrome confirms the well-known idea of the outstanding English scientist H. Jackson that localizing a symptom and localizing a lesion are not the same thing
So, neuropsychology is a discipline that significantly complements neurology, psychology, psychiatry, and linguistics.
It was the necessary link that made it possible to consider the human psyche in accordance with its cerebral organization - in its entirety, including those complex forms of behavior that had previously remained undisclosed in this form.
Factors influencing neuropsychological assessment
Neuropsychological assessment aims to provide a picture of changes in behavior that occur as a result of changes in the brain. Ideally, the conclusions from the tests used should not depend on factors that do not relate to aspects of brain functioning. Unfortunately, this is not always the case, because many external factors can influence test results. These include variables such as age, education, physical fitness. disorders, intelligence and mental. status.
Age
Tests that are sensitive to brain damage also show a generally high sensitivity to the effects of maturation and aging. Some believe that age-related effects are caused by brain changes that accompany aging; thus summing up the theory. basis for the observed sensitivity of neuropsychological tests to such effects. This sensitivity obliges neuropsychologists to consider age effects when analyzing test performance. It is also important to carefully analyze the results from this point of view. patterns of test performance that indicate brain damage but are masked by age-adjusted scores. The patterns observed under different conditions are not modified by age.
Children's performance on neuropsychological tests varies greatly by age. In addition, brain damage causes very different effects in children depending on their age. Ball, based on his own observations, came to the conclusion: the earlier the child’s brain is affected, the more severe the neuropsychological consequences.
Dr. An important challenge in children is to separate problems caused by developmental delays and mental retardation from problems caused by actual brain damage. In many cases, such a distinction cannot be made and, in practice, it is often irrelevant to the treatment plan.
Education
The role of educational level in test results is controversial. Upon closer inspection, it becomes apparent that many tests require a minimum level of education. The observed effects of education may be related to overall IQ, since individuals moving to each successive level of education appear to have a higher average IQ. This relationship, as well as the influence of educational level on commonly used tests, requires broader investigation.
Physical disorders
Peripheral impairments that impair motor skills, especially hand and mouth movements, can in many cases significantly affect the accuracy and validity of a number of neuropsychological tests. When working with such patients, it is often necessary to replace tests widely used in neuropsychology with other tests that are insensitive to the level of motor coordination.
Intelligence
People with reduced intelligence perform less well on neuropsychological tests than do people whose intelligence is considered normal. Interpretation of results should be adjusted based on the patient's expected level of test performance.
Emotional problems
A major challenge in the assessment of organic brain dysfunction has always been the separation of deficits caused by brain damage from deficits caused by functional disorders. In many cases, the level of test performance demonstrated by an individual with a chronic functional disorder is indistinguishable from that of a patient with a disorder of organic origin. Therefore, it is often necessary to use alternative diagnostic procedures to distinguish between such cases.
One important difference between patients with organic brain damage and those with schizophrenia concerns consistency in test performance. Patients with organic disorders show high consistency in the areas where they have deficits. Patients with functional disorders, on the contrary, may demonstrate high variability of results. Dr. An important strategy is to examine the test results for patterns of performance consistent with brain damage. Although a schizophrenic may demonstrate decreased performance on a test, it is rare that such decreased performance will indicate a specific organic disorder, as is typically the case in a patient with a specific organic brain syndrome. A final strategy is to try to minimize the decline in test performance in patients with functional disorders by organizing shorter testing sessions to maximize motivation to perform and minimize fatigue. In addition, changes in drug treatment for these patients can significantly improve test performance.
Experimental neuropsychology
Clinical neuropsychology receives considerable attention, but experimental research is an equally important area. N., who studies both people and laboratory animals, tries to identify the relationship between the brain and behavior. Where it comes to research. in public, between experiments. human neurophysiology and clinical neurophysiology there is a very fine line. However, the goals of the two areas differ significantly. While clinical neuropsychology attempts to find rules and procedures that are effective in working with large numbers of patients, often with unspecified (and indeterminate) disorders, experimental. neuropsychology of people systematically studies patients with well-defined and limited disorders to advance our knowledge of the relationship between brain and behavior.
View all Articles