Diseases of the human central nervous system are spreading more and more with the modern, unnatural way of life. Constant stress, overwork, poor and sedentary lifestyle – all this increases the risk of neurological pathologies, which can be fatal. One of the most common diagnoses in this area, which in the European part of Russia in terms of quantitative indicators is at least twice the world level: the disease is diagnosed in 25-50 people per 100 thousand, is multiple sclerosis.
It has its own cycle associated with the gradual fading of the ability to work and, unfortunately, to live. For working people, disability due to multiple sclerosis is becoming the norm. In today's review, we will look at what disability group is assigned to multiple sclerosis, how it is established and confirmed, and also answer other common questions about life activity and risk associated with this diagnosis.
Origin and development of the disease
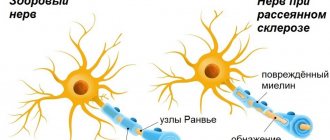
Multiple sclerosis is a chronic disease classified as autoimmune. As the disease progresses, it inevitably leads to disability, destroying human health in many ways. The main violations appear:
- loss of vision;
- hearing loss;
- paralysis of arms and/or legs;
- a general decrease in sensitivity to all stimuli.
MS can begin to appear in people of almost any age. The average starting age range is from 15 to 45 years; both children and old people can suffer from multiple sclerosis. In the initial stages, the disease is asymptomatic. Therefore, you need to monitor the manifestations of certain signs:
- blurred vision;
- problems with the vestibular system: dizziness, loss of balance and stability;
- problems with coordination of movements;
- slower reaction;
- general weakness;
- the presence of spasms and/or convulsions in the body.
All this may indicate the onset of MS, which cannot be stopped - the disease will progress and worsen. The presence of multiple sclerosis can be diagnosed based on the results of an MRI of the brain under the supervision of a neurologist. The presence of the disease can be assumed, but the diagnosis must be confirmed clinically. The disease can develop according to several scenarios, depending on the form of its course:
- relapsing or remitting. Remissions (can last a year or even several years) are interspersed with acute phases. “Gray matter” after damage is capable of both partial and complete restoration of the functions of the affected areas;
- primary progressive. A smooth but unstoppable trend of health deterioration, which, in the absence of acute phases, on average makes a person incapacitated twice as quickly;
- secondary progressive. In the early stages, it is very similar to the typical recurrent form, which subsequently develops into a continuously progressive one;
- progressive-remitting. It is the least common and combines the first two types. Parts of the brain that survive the attack do not regain their functions.
The disability group for multiple sclerosis is almost directly dependent on the stage at which the disease is located. There are four of them in total and are called ordinal numbers (from 1 to 4):
- The human central nervous system shows initial signs of a functional disorder, while continuing to operate generally stably;
- lesions of the central nervous system partially affect the organs of vision, reduce hearing, and impair coordination of movements;
- The central nervous system exhibits disruptions in its basic functions, the person loses attention and fine motor skills, and becomes tired above average;
- terminal stage of central nervous system depression. The patient is almost or completely unable to see, hear, or move. Can move around in a wheelchair and requires constant care.
What specific disability group can be obtained with multiple sclerosis?
There can be three groups in total, one of which you can count on:
- The first group includes patients who have serious vision problems, and also have disorders in the functioning of the musculoskeletal system, usually in the form of local paralysis
- The second group is assigned to those who have noticeable motor dysfunction and other accompanying disorders
- The third group includes those patients who are almost fully functional, but have innervation disorders
Depending on the degree of disability assigned to the patient, he will receive appropriate government payments for this.
Their sizes are as follows:
- 1 group – 9,919 rubles
- Group 2 – 4,959 rubles
- Group 3 – 4,215 rubles
- Group 4 (concerning children with disabilities) – 11,903 rubles
Concentrated therapy
MS is incurable, but competent therapy will help prolong remissions and reduce the manifestations of the disease. The adequacy of treatment directly affects the duration and quality of life of patients with multiple sclerosis; it is selected individually (depending on the severity, stage, form, manifestation of MS). The most common treatment methods are:
- taking steroids and cytotoxic drugs;
- blood plasmapheresis;
- use of immunosuppressants and immunomodulators;
- use of interferons;
- suppression of symptoms (taking antioxidants, amino acids, vitamins, nootropic drugs, enterosorbents, muscle relaxants, vascular therapy, etc.);
- hormone treatment;
- rehabilitation in remission (physical therapy, massage, sanatorium treatment courses).
Reducing to disability
Multiple sclerosis definitely implies disability, starting from the third stage, but which group - the decision is made based on the results of a comprehensive study.
The first stage of the disease is not a sufficient basis for registration of disability, but it is already recommended to choose easier work, minimizing eye strain, joints and physical overload.
Whether disability is due to multiple sclerosis - the answer is given by a collegial decision of an expert commission (medical and labor) based on the results of the examination. The commission may allow a disabled person to work in professions allowed with MS, or assign a “non-working” group. The commission may award one of three degrees designed for disability:
- Group III – “working”. Assigned for minor impairments in the ability to move;
- Group II – with obvious symptoms of damage;
- Group I – with the appearance of extreme impairments and loss of the ability to move independently.
The nature of the disability is established as indefinite if doctors determine the impossibility of improvement in the condition of a patient who is unable to work.
To convene a VTEK, criteria are needed, which are usually:
- the patient's inability to perform his or her job fully;
- lack of effect from treatment for multiple sclerosis (a person may receive inpatient or outpatient treatment but show no improvement);
- disease progression;
- temporary disability due to MS for four months or more.
Depending on the situation and the patient’s condition, the commission carries out its work in a medical institution, at the patient’s home or in his hospital ward. The conclusion on the need for examination for disability is given by the attending physician.
Initial signs of the development of multiple sclerosis
The risk group for multiple sclerosis is teenagers, young adults and middle-aged people. The disease leads to damage to the central nervous system, which does not allow one to fully perform one’s duties and leads to a deterioration in the patient’s quality of life. Initial signs of the development of the disease may appear in the form of visual impairment:
- The patient feels a foreign body in the eye.
- A veil appears before the eyes, the image becomes fuzzy and cloudy.
- The patient may lose visual color perception, not distinguish between colors or just one color.
Such visual impairment may occur in one or both eyes. Symptoms last for several days and then disappear. The patient may experience pain when moving the eyeballs, when pressing on the eye, and increased sensitivity to bright light. Other symptoms of multiple sclerosis include impaired calligraphy, inability to make coordinated movements of the legs and arms, general unsteadiness of the body, sensory disturbances, and urinary retention or frequent urination. The disease can manifest itself as depression, irritability, constant fatigue, and memory impairment.
Examination rules
The development of MS led to the inability to work in the same place. Do multiple sclerosis provide disability in this case - we discussed above. Now let’s present a confirmation mechanism, a list of reasons for the work of VTEK. For a commission examination there must be:
- Diagnosis confirmed. MS is determined based on the results of a comprehensive examination required in such cases, including (at a minimum):
- identification of affected areas of the central nervous system - MRI of the head and spinal cord;
- determination of the state of immunity - analysis of capillary and venous blood;
- determining the condition of the spinal cord - performing a lumbar puncture;
- determination of the state of hearing and vision - the conclusion of an ophthalmologist and otolaryngologist;
- determining the reaction to an injection of the Margulis-Shubladze composition (a positive reaction can be confirmation of the presence of the disease).
- The treatment course intended for the patient has been completed.
- The attending physician's verdict on the need for MSA was issued. This conclusion is due to the low effectiveness of treatment, poor recovery of damaged areas, and a negative prognosis for the development of MS.
The commission itself evaluates the person’s condition based on the results of studying the research results. The following are taken into account: problems with the patient’s speech and swallowing reflex; the functioning of internal organs and the presence of enuresis/involuntary bowel movements; mental state, etc. Each indicator is the basis for assigning points on a scale designed specifically to determine disability, including for patients suffering from various forms of a disease such as multiple sclerosis.
The process of making a decision on the assignment of disability takes from 4 months to a year, and it is necessary to overcome the acute phase of the illness. Upon re-examination, neurologists can increase the category of disability or, on the contrary, remove restrictions - it all depends on the course of MS and changes in the patient’s condition.
Multiple sclerosis: instrumental diagnostics when referred to MTU
Definition: Multiple sclerosis is a chronic progressive disease of the central nervous system, characterized by multifocal lesions of the white matter of the brain and spinal cord.
The socio-economic and medical significance of MS is very great, because People of the most productive age are excluded from active life for a long time. It is worth noting that a large percentage of citizens applying for examination to the federal state institution “Main Bureau of Medical and Social Expertise for the Republic of Tatarstan” (hereinafter referred to as FSI “GB MSE for the Republic of Tatarstan”) are sick with multiple sclerosis.
In 2009, the ITU Bureau No. 20 of the Federal State Institution “GB ITU for the Republic of Tatarstan” examined a total of 22 patients with the disease “Multiple Sclerosis”. At the same time, there are 2 cases of initial examination to determine the disability group. Of the 20 cases of re-examination, 4 are examinations regarding the development of an individual rehabilitation program for a disabled person.
Gender distribution: 19 women and 3 men. At the same time, there are 16 women under 45 and men under 50. Among the disabled, city residents predominate - 18 people, village residents - 4 people. At the same time, there are 14 citizens of mental labor. Distribution by disability groups: first - 4, second - 13, third -5.
The diagnosis of MS continues to be based primarily on clinical findings. There is no pathognomonic laboratory test or instrumental examination that allows an unconditional diagnosis of PC.
Next, we will consider the instrumental research methods that were carried out on these patients when they were sent for examination to the ITU bureau. Some of these examinations are crucial in making a diagnosis of Multiple Sclerosis; other examination methods were carried out in combination to clarify concomitant diseases or were included in the examination standard. Conducted: magnetic resonance imaging of the brain, magnetic resonance imaging of the spinal cord, visual evoked potentials, acoustic brainstem evoked potentials, somato-sensory evoked potentials, computed tomography of the brain, electroencephalography, electroneuromyography, duplex scanning of the main arteries of the head, rheoencephalography, ultrasound examination abdominal organs, fibrogastroduodenoscopy.
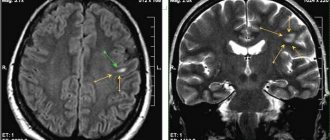
Magnetic resonance imaging (MRI) is the most informative and accessible study confirming the diagnosis of PC.
Of the 22 examined, 20 patients underwent MRI of the brain. Two patients who did not undergo MRI had a long history of illness and a significantly pronounced neurological deficit. They have been disabled for a long time in the first group and have been examined for the development of IPR (technical means of rehabilitation). Moreover, one of these patients underwent computed tomography of the brain in 2002. When analyzing the examination case at ITU (VTEC), there were no references to MRI. The remaining twenty disabled people underwent MRI in different years. Three patients underwent this examination in the year of examination (2009). One year before the last survey (2008) there was one case. In 2007, 4 MRIs. In 2006, 5 MRIs of the brain. In previous years in the remaining 7 cases. Repeatability of the examination during observation at the ITU: once - 11 cases, twice - 5 cases, three or more - 4. MRI of the brain was combined with MRI of the spinal cord in three cases; CT scan of the brain - in two patients. Pathological changes in the MR signal were observed in almost all observation cases. The nature of the description of these changes varies depending on the year of the examination, the medical institution in which the examination was carried out, the resolution of the device, and the doctor who carried out the description. The most commonly described are multiple foci of demyelination and changes in the intensity of the MR signal. The primary localization of the process is periventricular, in the white matter of the cerebral hemispheres.
The number, size and location of lesions weakly correlate with clinical symptoms, the degree of disability of the patient and provide very poor information regarding the prognosis.
Computed tomography of the brain: this examination was performed in 4 patients. In one case there is no pathology. An arachnoid cyst, moderate hydrocephalus, and in one case, foci of degenerative changes in the temporal lobe were revealed? ischemic in nature?
Visual evoked potentials: examination was carried out on 8 recipients, one – twice. In only one case no pathology was detected. In all other examinations, the visual analyzer was found to be of the demyelinating type.
Acoustic brainstem evoked potentials: examination was carried out in 2 patients: dysfunction of acoustic structures was revealed.
Somatosensory evoked potentials: examination was carried out in 2 patients: demyelinating changes were revealed.
Non-invasive, safe and easy-to-perform evoked potential (EP) testing is usually not sufficiently informative in the diagnosis of MS. Using visual EPs, it is possible to detect involvement of the optic nerve in patients without symptoms of optic neuritis, but, unfortunately, the list of conditions that can cause similar changes in the latency and shape of the peaks of visual EPs is quite large
Electroencephalography was performed in one case: interhemispheric asymmetry.
Electroneuromyography was performed on two disabled people; conclusion: a neuronal process cannot be excluded.
The use of electroencephalography, electroneuro- and electromyography when MS is suspected does not seem rational, since their informative value in diagnosing MS is extremely low
Duplex scanning of the main arteries of the head: examination was carried out in 2 recipients. In one case, no pathology was detected. One patient had tortuosity of both VAs in the first and second segments.
Conclusions:
Among disabled people with multiple sclerosis, women of working age under 45 predominate. Citizens with secondary technical and higher education and people with mental work predominate. Only a quarter of disabled people with a work recommendation work. Seventy-five percent of disabled people have the first and second disability groups. Carrying out instrumental examination methods when referring citizens with the nosology “multiple sclerosis” to MSE is mandatory. It is necessary to take into account that the most informative are: Magnetic resonance imaging (MRI) of the brain and the study of evoked potentials (EP)
Head of Bureau No. 20 of the Federal State Institution “Main Bureau of Medical and Social Expertise in the Republic of Tatarstan” Ayrat Shavkatovich Khasanov
Doctor of the Functional Diagnostics Department of the Medical and Sanitary Unit of OJSC TATNEFT Venera Foatovna Khasanova