Signs of diabetes
If you are overweight, constantly feel thirsty, have sudden changes in blood pressure, and your vision has noticeably deteriorated, then you should think about whether diabetes mellitus is the cause of these symptoms. Diabetes mellitus detected in the early stages helps to start treatment on time and eliminates possible complications.
How does diabetes affect potency?
How does diabetes mellitus have such a negative effect on potency? This process is quite complex, so we will conditionally divide it into several points.
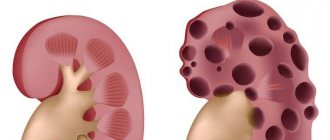
Vessels
Veins and arteries become narrow and stiff due to glucose deposited on the walls. The body cannot fully perform the function of blood supply to the pelvic organs and blood vessels of the penis. Arousal takes more and more time, and erections become weak.
Nervous system
It is responsible for the tone of the urinary tract and erection. With diabetes mellitus, erectile dysfunction occurs, chronic inflammation of the genitourinary tract and premature ejaculation are possible.
Diabetes mellitus is a disease that seriously affects the brain. Depression and frequent mood swings are likely, which also have a negative impact on your intimate life.
Glands that produce hormones
The glands that produce hormones reduce the production of testosterone (the male hormone) and thyroxine (the thyroid hormone), due to increased blood sugar levels. The result of reduced production of these hormones is a decrease in libido and erection.
Immunity
There is a decrease in the overall tone of the body and a strong weakening of the immune system. Fatigue, noticeable weakness, inflammation of the tissues and pelvic organs become more frequent with diabetes.
Despite the danger of a disease such as diabetes, we can stop the deterioration of potency.
Impotence in diabetics: can it be avoided?
But with the right approach and drug treatment, this problem can be avoided altogether or at least reduced the risk of impotence. Our clinic specialists will help you with this. We have extensive experience, knowledge, as well as modern equipment and innovative programs in the treatment of various diseases.
Impotence in diabetes: causes
As we have already said, impotence is quite common in men with diabetes. Moreover, it appears even in young people. In 25% of diabetics, this disease is diagnosed at the age of 30-40 years, in 55% of cases - in 50-60 year old men, and at the age of 65-70 years, 75% of diabetics are already doomed to impotence.
What are the causes of decreased sexual function in men with diabetes? Our doctors highlight several:
- Hormonal disorders. It is no secret that diabetes mellitus affects the functioning of all organs and systems of the human body. Diabetes is an endocrine disease; its root cause is a disruption in the production of many hormones in the body, including sex hormones (testosterone). But the duration of sexual intercourse, the time and strength of an erection depend on its quantity. This leads to periodic and subsequently permanent problems in intimate life.
- Changes in the amount of sugar in the blood. Moreover, men’s health is affected by both a decrease in glucose levels and an increase. Such changes occur several times during the day, even in a healthy person. In a diabetic, the fluctuations are much more extreme, so they need to be monitored carefully. Our experts warn that low sugar levels interfere with the active functioning of those centers of the brain and spinal cord that are responsible for erectile strength and ejaculation. Therefore, diabetics suffer from a complete lack of ejaculation or, conversely, from prolonged ejaculation. If the brain is not properly nourished, sexual desire may subsequently disappear altogether. But still, doctors consider the main enemy of male power to be an increase in glucose levels, the molecules of which slow down the reaction of nerve endings that lead to the genital organ. In men with diabetes, as a rule, the sensitivity of the scrotum, head of the penis and the entire perineum is reduced.
- Vascular damage. Diabetes mellitus leads to injury to blood vessels throughout the body. As a rule, small capillaries are the first to suffer, including the vessels of the genital organ. Because of this, circulatory disorders in this area are common. When excited, the penis does not fill with blood sufficiently, which leads to a weak erection and incomplete sexual intercourse.
How to avoid impotence with diabetes
Fortunately, it is possible to reduce the risk of impotence in diabetics. Using various procedures, medications and lifestyle adjustments, our specialists will help you fight this problem. Come to our clinic - a doctor’s consultation and timely treatment will help you improve your intimate life and reduce the negative impact of diabetes on your virility. Most importantly, you need to constantly monitor your blood sugar levels and take medications that regulate the amount of glucose in a timely manner.
Since diabetes progresses quickly, our doctors often prescribe insulin therapy, which helps maintain constant blood sugar levels and avoid sudden changes.
In addition, we will help you create a balanced and healthy diet to avoid complications that are often observed in patients with severe compensation of the disease.
For people suffering from diabetes, we can offer a program that helps restore erectile function and avoid problems in the sexual sphere. Here are some recommendations from our experts:
- give up bad habits, don’t drink alcohol, don’t smoke;
- play sports at least several times a week, try to walk more, lead an active lifestyle;
- follow the diet suggested by our clinic doctors to maintain a constant blood glucose level;
- control “bad” cholesterol, this will help avoid problems with blood vessels;
- watch your weight;
- Measure your blood pressure daily.
Following these recommendations will normalize erectile function and improve the quality of your life, including its sexual side.
Examinations of men with diabetes mellitus
Diagnosis of impotence in diabetes mellitus includes a number of procedures:
- hormonal studies to determine the level of prolactin, extradiol, LH, FSH, thyroid-stimulating hormone and testosterone;
- assessment of lipid spectrum;
- a physical examination carried out to determine the vibration and tactile sensitivity of the penis, scrotum, and perineum.
Treatment of erectile dysfunction
Treatment of impotence in patients with diabetes is carried out using the latest medical advances. Our specialists use various approaches and methods to correct erectile function in men:
- drug therapy;
- LOD therapy, which is a massage using special vacuum erectors;
- an experienced psychotherapist conducts psychotherapy sessions, which are one of the important points in the treatment of impotence;
- If necessary, surgical intervention is performed: vascular surgery, prosthetics of the genital organ.
Thanks to their extensive experience and extensive knowledge, the doctors of our clinic in most cases cope with this problem, patients experience positive dynamics and a significant improvement in their condition.
Improving potency in diabetes mellitus
If you notice symptoms and signs of diabetes, consult your doctor immediately. A specialist will examine you and conduct some investigations that will show whether treatment is necessary.
Follow your doctor's advice, this will help you in the fight against decreased potency. Try to get rid of bad habits: smoking and alcohol. An active lifestyle and proper nutrition are also necessary to maintain health.
The doctor must prescribe you special medications that you must take regularly, without missing a single dose. An effective and safe means to increase potency can be the drug Prosta-Vita.
The drug Prosta-Vita is made from natural ingredients of plant and animal origin. The action of the drug is aimed at making sex for a man again desirable and enjoyable.
Following these simple recommendations guarantees you an improvement in potency and an increase in the quality of your intimate life.
Erectile dysfunction in patients with type 1 diabetes: methods of diagnosis and treatment
Kurbatov D.G., Dubsky S.A., Lepetukhin A.E., Rozhivanov R.V., Shvarts Ya.G.
Federal State Budgetary Institution Endocrinological Scientific Center of the Ministry of Health of Russia, Moscow Address: 117036, Moscow, Dm. Ulyanova St., 11, tel. (499)3203687 Email
Introduction
The incidence of diabetes mellitus in the world is rapidly increasing. According to the International Diabetes Federation, today more than 371 million people suffer from diabetes mellitus (DM). Approximately 10% of the total number of patients with diabetes are type 1 diabetes [1].
Sexual disorders, characterized by a decrease in the patient’s quality of life, leading to infertility and social problems, are observed in more than 40% of patients with diabetes [2, 3]. It is important to note that sexual disorders in patients with type 1 diabetes begin at a younger age compared to the population without diabetes [4].
The prevailing sexual dysfunction in patients with diabetes is erectile dysfunction (ED). Numerous studies have shown that ED affects up to 35-55% of patients with type 1 diabetes [5], and the risk of ED in patients with diabetes is 3 times higher compared to the population without diabetes [6].
The incidence of erectile disorders in patients with diabetes depends not only on the patient’s age, but also on the duration of the underlying disease and the duration of the period of decompensation of carbohydrate metabolism [7, 8]. The development of ED is influenced by the presence of concomitant diseases, complications of diabetes, and the effectiveness of the therapy [9]. Thus, several studies have examined the relationship between the presence of ED and late diabetic complications and have shown that ED was detected almost 2 times more often in patients with diabetic nephropathy or retinopathy [10].
Diagnosed erectile dysfunction in patients with diabetes may be an indirect sign of the development or progression of the atherosclerotic process and coronary heart disease, and may also be the first manifestation of diabetic neuropathy [11, 12]. A similar study conducted by Rozhivanov R.V. (2005) on the basis of the Federal State Budgetary Institution "Endocrinological Scientific Center" of the Ministry of Health of the Russian Federation, shows comparable with foreign data on the prevalence of ED among patients with type 1 and type 2 diabetes, the dependence of the prevalence on the age of patients, the duration of the disease, as well as the relationship with the level of compensation of carbohydrate metabolism and the presence complications of diabetes [13].
Considering the prevalence of ED in type 1 diabetes, as well as the understanding that this condition not only reduces the quality of life of young patients, but can also be one of the symptoms of diabetes complications such as diabetic neuropathy, coronary artery disease, atherosclerosis, a timely, individualized and comprehensive approach is required to the diagnosis and treatment of ED in this category of patients.
Classification of ED
ED forms:
- Organic (vasculogenic, neurogenic, endocrine)
- Psychogenic
- Mixed (organic pathology and psychological factor)
- Medication
The functional state of the penis is regulated by the tone of the smooth muscles of the arterial vessels and trabeculae of the cavernous bodies. After sexual stimulation, nitric oxide (NO), produced by the endothelium, increases the concentration of guanylate cyclase (GMP). Increasing concentrations of cyclic GMP (cGMP) lead to relaxation of smooth muscle fibers, increased arterial inflow and veno-occlusion in the penis. The rate of cGMP breakdown depends on the activity of the enzyme 5-phosphodiesterase [14].
The development of ED in diabetes may be based on several factors simultaneously (atherosclerosis + neuropathy, neuropathy + psychogenic factor, etc.) [15].
Penile erection is regulated by various isoforms of NO synthetase of neuronal, endothelial and smooth muscle origin. [16]. Several biochemical mechanisms explain the occurrence of erectile dysfunction in diabetes. The vascular and neurogenic components together are the causes of ED in diabetes, since it is known that endothelial dysfunction leads to the development of ischemic neuropathy, which, in turn, has a negative effect on NO synthesis. Many studies have shown impaired endothelial-dependent and neurogenic relaxation in the corpora cavernosa in patients with diabetes and ED. This finding is associated with NO deficiency. Moreover, some foreign studies have shown a significant increase in the number of NO-synthetase-binding sites in the tissues of the corpora cavernosa of rats 2 months after the induction of diabetes mellitus [17]. This process is similar to those found in other vascular beds, where endothelium-dependent relaxation of the vascular wall was altered as a result of impaired NO synthesis due to high glucose concentrations. Thus, a defect in NO synthetase activity plays a role in the etiology of ED in patients with diabetes, due to diffuse endothelial dysfunction [18]. It was also shown that the relaxation of smooth muscle cells in the corpora cavernosa in patients with diabetes during electrical stimulation was weak due to a decrease in the production of nitric oxide by NO synthetase. It is important to note that long-term hyperglycemia induces an increase in the consumption of nicotinamide adenine dinucleotide phosphate (NADPH), a cofactor in NO production, consequently reducing nitric oxide levels [19].
Excessive generation of free radicals impairs NO-induced relaxation and through the accumulation of advanced glycation end-products (AGEs) circulating in the blood, which are also responsible for the development of diabetic vascular complications [20].
AGE products, accumulating in patients with diabetes, interact with specific tissue receptors that are exposed to vascular damage, and also increase the expression of mediators of vascular damage, the release of which is also stimulated by glucose. [21, 22, 23].
All of the above factors are involved in the pathophysiology of cardiovascular diseases characterized by high mortality (silent myocardial ischemia, sudden cardiac death, etc.), which are highly associated with ED [24].
Neuropathy is an important component in the development of diabetic ED. Morphological damage to autonomic nerve fibers in the tissues of the cavernous bodies in patients with diabetes and ED has been shown [25]. The presence of peripheral polyneuropathy is considered characteristic of patients with ED, however, a decrease in the speed of nerve impulses along the nerve fiber and heart rate variability are still recorded slightly more often in patients with diabetes and ED than in patients with ED and polyneuropathies of other origins [26].
Numerous studies devoted to pathological changes in the nervous system in patients with diabetes indicate independent primary damage to peripheral nerve fibers [27].
Autonomic neuropathy appears to be the main pathogenetic factor of ED in patients with diabetes. Patients with manifestations of peripheral neuropathy more often suffer from ED than patients with diabetes without polyneuropathy [28]. The most substantiated metabolic hypothesis is the theory of polyol metabolism, according to which excess glucose in diabetes is metabolized according to the polyol type, ultimately turning into sorbitol and fructose, the accumulation of which in nerve cells triggers the development of neuropathy [29]. The significance of hyperglycemia in the development of diabetic neuropathy is clinically confirmed by the fact that, provided that compensation of carbohydrate metabolism is achieved, the progression of diabetic neuropathy is reduced by 40-60% [30].
The vasculogenic hypothesis for the development of neuropathy, based on depletion of endoneural blood flow, increased endoneurial vascular resistance and decreased oxygenation of the nerve, is also important. According to this theory, the primary pathological changes in endoneurial vessels and associated hypoxia and ischemia [31].
All of the above indicates the important role of peripheral neuropathy in the development of ED in patients with diabetes. Many authors characterize this condition as “neurogenic ED,” thereby drawing attention to the leading role of diabetic neuropathy in erectile disorders in such patients [31, 32].
Along with vasculogenic and neurogenic forms of ED in diabetes, endocrine ED associated with androgen deficiency is common [33].
Recent studies have demonstrated that NO synthetase is an androgen-dependent enzyme [34]. The androgen dependence of NO synthetase is evidenced by the fact that androgen receptors are found in the nerve cells of the pelvic parasympathetic ganglia, in which the synthesis of NO and vasoactive intestinal peptide occurs [35], as well as stimulation of NO synthesis in the ganglia under the influence of androgens [36]. Moreover, hypogonadism is a common symptom in patients with diabetes [37]. The causes of androgen deficiency in men with diabetes are different. These reasons may be overweight or obesity, as well as an age-related decrease in testosterone secretion. [38].
Diagnosis of ED in patients with diabetes
Examination of a patient with ED in diabetes is carried out according to the classical scheme, including the collection of anamnestic data, examination, as well as laboratory and instrumental methods.
An important point in collecting anamnesis in patients with diabetes is to assess the course of the underlying disease, the presence or absence of complications of diabetes, and information about medications taken.
During the physical examination, weight, height, and body mass index are measured, as excess weight can cause hypogonadism. In some cases, it makes sense to conduct a differential assessment of the volume of visceral fat using CT scanning for a more correct assessment and prediction of risks. In addition, the condition of the skin, the nature and intensity of hair growth, the condition of the muscular system and genital organs are assessed [39, 40].
During a physical examination, in order to diagnose neuropathy, it is necessary to perform a certain minimum of neurological diagnostic techniques. The most informative is the assessment of the cavernous reflex [41]. An assessment of the temperature, tactile and vibration sensitivity of the penis may also be recommended [42].
The list of special examination methods for ED includes hormonal blood testing, monitoring of nocturnal penile tumescences, intracavernosal pharmacodynamic study, cavernosography, angiography of penile vessels, Doppler ultrasound of penile vessels and determination of the speed of propagation of nerve impulses according to n.pudendus [43].
All of the above examination methods are used to diagnose ED of any origin, however, the most informative and currently only reliable method for diagnosing the neurogenic form of ED in diabetes is electroneuromyography. Tests that assess the condition of sensory and efferent fibers include perineal electromyography of the bulbocavernosus reflex latency period, sacral latent test, assessment of dorsal somatosensory evoked potentials, and vibration perceptual sensitivity testing. Patients with diabetes and ED are characterized by deviations of the results of these tests from normative indicators. For example, patients with diabetes are characterized by an increase in the latent period of the bulbocavernosus reflex [43]. However, the tests described above do not provide an idea of the state of the efferent autonomic innervation responsible for penile erection. Based on the above, when recording test results that are abnormal, one can only assume the presence of autonomic neuropathy in the penis [44].
As a method of direct study of the autonomous cavernous innervation, the electrical activity of cavernous smooth muscles can be recorded using intracavernous or superficial cutaneous electrodes. Data obtained using this method make it possible to assess the state of the neuro-reflex function of the penis and identify disorders at the level of interaction between the cavernous bodies and nerve endings. When studying the autonomous cavernous innervation in patients with diabetes, irregular potentials with low amplitude and slow depolarization rates are recorded, and desynchronization is also characteristic - a paradoxical increase in the activity of cavernous tissue in response to the administration of a vasoactive drug, while in healthy patients after intracavernous administration of vasoactive drugs there are no action potentials [45]. Currently, there is insufficient data regarding the specificity and sensitivity of this method.
Based on the foregoing, it becomes clear that diagnosing the actual neurogenic form of ED in patients with diabetes is a difficult task, especially considering that today there is no highly sensitive and specific diagnostic method. It should be taken into account that erectile dysfunction is often the first symptom of developing neuropathy. A neurogenic form of ED in a patient with diabetes can be assumed in the presence of other manifestations of diabetic neuropathy (decreased temperature, vibration and pain sensitivity, various manifestations of cardiovascular and gastrointestinal forms of autonomous diabetic neuropathy, unrecognized hypoglycemia). The absence of evidence for the presence of vascular insufficiency and hypogonadism, along with complaints of erectile disorders, may also indicate neurogenic ED.
Treatment of ED in patients with diabetes
When choosing a treatment method for ED, each patient requires an individual approach [45]. Considering the possibility of specific complications in patients with diabetes, the choice of treatment methods for ED should be justified [46]. As you know, the use of drug treatments for ED is currently preferable, but what is even more important: for effective treatment of ED it is necessary to achieve stable compensation of carbohydrate metabolism.
Today, there are a number of methods for local treatment of ED: vacuum therapy, intracavernous and transurethral pharmacotherapy. All these methods have certain disadvantages that limit their use in patients with diabetes, as they are associated with possible trauma to soft tissue during intracavernous pharmacotherapy and the urethral mucosa during transurethral pharmacotherapy, which is undesirable for patients with diabetes due to the high risk of infection of microtraumas [45].
Currently, the drugs of choice for the treatment of ED are phosphodiesterase type 5 inhibitors (sildenafil, vardenafil, tadalafil, udenafil). Drugs in this group are erection modulators that selectively inhibit the PDE-5 enzyme, without directly affecting the smooth muscle cells of the penis, but enhancing the effect of NO, which is synthesized in response to sexual stimulation. Thus, the physiological processes responsible for the occurrence and maintenance of an erection in response to sexual stimulation are enhanced [45].
Many years of experience with the use of sildenafil in patients with diabetes has demonstrated its high effectiveness in the treatment of ED [46, 47]. This is evidenced by long-term studies, the results of which indicate the possibility of long-term, safe, effective use of the drug without increasing its dose [48].
The effectiveness of vardenafil in the treatment of ED in patients with diabetes was studied in a multicenter, double-blind, placebo-controlled study that included 452 patients. According to the evaluation of the study results, after 12 weeks of use, improvement in erection was observed in 52% and 72% of men receiving 10 and 20 mg of vardenafil, respectively, while in the placebo group, improvement in erection was observed in only 13% of patients [49].
The effectiveness and safety of tadalafil in men, including patients with diabetes, was studied in a study by Fonseca V. et al. (2006), which conducted a meta-analysis of data from twelve placebo-controlled studies in patients with ED, diabetes and without it. The studies included 1,681 men without diabetes and 637 men with type 1 and type 2 diabetes who received tadalafil 10 mg, 20 mg, or placebo for 12 weeks. Patients with diabetes had more severe ED than patients without diabetes, and the IIEF ED score was inversely correlated with HbA1c levels. Compared with placebo, tadalafil in doses of 10 and 20 mg significantly improved erectile function in both groups, which was accompanied by an increase in the quality of life of patients. Moreover, the effectiveness of tadalafil did not depend on the degree of compensation of carbohydrate metabolism and the therapy received for diabetes. Thus, despite more severe ED in patients with diabetes, tadalafil was effective and well tolerated [50]. Tadalafil has a long half-life of 17.5 hours, which ensures a significantly longer duration of action, returning naturalness to sexual relations [51]. The patient has the opportunity to lead a natural sexual life, which is extremely important in the presence of additional psychogenic factors that aggravate the course of erectile dysfunction in patients with diabetes [52].
According to researchers, in 20-40% of patients with ED, therapy with PDE-5 inhibitors is ineffective, which in some cases is due to the presence of androgen deficiency in patients. Thus, in some cases, it seems advisable to prescribe combination therapy with androgens and PDE-5 inhibitor drugs from the moment of diagnosis to patients with the above-described clinical features, which increases the effectiveness of therapy to 93% [53, 54, 55].
The use of PDE-5 inhibitor drugs in the treatment of sexual dysfunction in patients with diabetes may have the additional benefit of reducing the symptoms of genital neuropathy [49]. Thus, in a study that included 16 men with type 1 diabetes and ED at the age of 27 [25;29] years with paresthesia in the shaft of the penis and impaired sensitivity of the glans, receiving a PDE-5 inhibitor for 3 months, not only complete elimination of ED in all patients (ED score during therapy 21 [21;22], p<0.001) and normalization of spontaneous erections, but also a statistically significant reduction in complaints characteristic of genital neuropathy, as well as improvement in the temperature sensitivity of the penis [49] .
The neuroprotective effect of PDE5 inhibitors has been noted in diabetic neuropathy. The publication by G. Hackett describes 5 clinical cases where patients with a painful form of distal diabetic neuropathy noted a significant decrease in the severity of symptoms after regular use of PDE-5 inhibitors. The beneficial effects of PDE5 inhibitors can be explained by their effects on endothelial function by improving blood flow through the vasa nervorum [56].
Until now, alpha lipoic (thioctic) acid preparations have been the most promising for the treatment of painful forms of diabetic polyneuropathy [57]. A number of foreign and 1 domestic non-placebo-controlled study have shown the effectiveness of these drugs in the treatment of both diabetic polyneuropathy in general and neurogenic ED in particular. However, it should be taken into account that the effect was short-term and was determined by the time of intravenous infusions [58].
Despite a fairly wide choice of drugs for conservative treatment of ED in patients with type 1 diabetes, there is a group of patients in whom these treatment methods remain ineffective. In this case, patients are indicated for surgical treatment - penile endoprosthetics.
Conclusion
This literature review covers issues of epidemiology, classification, pathophysiology, as well as diagnosis and treatment methods for ED in patients with type 1 diabetes. ED in young patients with diabetes is a serious problem due to its fairly wide prevalence, as well as its impact on the psychological state of patients and quality of life in general.
From all of the above, it becomes clear that today a doctor has a wide range of different methods for diagnosing ED, but a highly specific and sensitive method for diagnosing the neurogenic form of ED has not yet been developed. It is important to consider that timely diagnosis with the correct determination of the form of ED allows you to reasonably and adequately select therapy for each individual patient.
Treatment of ED in patients with type 1 diabetes should be comprehensive and aimed not only at improving erectile function itself, but also at eliminating pathogenetic factors in the development of ED, such as chronic hyperglycemia, dyslipidemia, and androgen deficiency. Currently, preference is given to drug treatment methods, the leading place among which is occupied by drugs from the group of PDE-5 inhibitors due to their high efficiency, safety and ease of use for patients. It is worth noting that drugs in this group have a neuroprotective effect, which is especially important for patients with the neurogenic form of ED, but this issue requires further in-depth study.
Thus, despite great achievements in the development of methods for diagnosing and treating ED, there are still many unresolved issues that require further research.
Literature
1. International Diabetes Federation [Internet]. Cited 2013 Dec 9. Url.: https://www.idf.org/worlddiabetesday/tool kit/gp/facts-figures.
2. Prevalence of erectile dysfunction and its correlates: a population-based study in Morocco / S. Berrada, N. Kadri, S. Mechakra-Tahiri, C. Nejjari // Int J Impot Res. – 2003. – Vol.15, Suppl 1. – P.3-7.
3. Prevalence and correlates of erectile dysfunction in a population-based study in Belgium / R. Mak, G. De Backer, M. Kornitzer, JM De Meyer // Eur Urol 2002. – Vol.41(2). – P.132-138.
4. Rozhivanov, R.V. Erectile dysfunction in patients with diabetes mellitus according to control and epidemiological studies / R.V. Rozhivanov, Yu.I. Suntsov, D.G. Kurbatov // Diabetes mellitus. – 2009. – No. 2. – P.51-54.
5. Bancroft, J. Erectile dysfunction in men with and without diabetes mellitus: a comparative study / J. Bancroft, P. Gutierrez // Diabet Med. – 1996. – Vol.13 (1). – P.84-89.
6. Schiel, R. Prevalence of sexual disorders in a selection-free diabetic population (JEVIN) / R. Schiel, UA Müller // Diabetes Res Clin Pract. – 1999, May. – Vol.44(2). – P.115-121.
7. Vinik, A. Erectile dysfunction in diabetes. / A. Vinik, D. Richardson // Diabetes Rev. – 1998. – Vol.6(1). – P.1633.
8. Sexual function in men with diabetes type 2: association with glycemic control / JH Romeo, AD Seftel, ZT Madhun, DC Aron // J Urol. – 2000. – Vol.163(3). – P.788-791.
9. Effect of chronic diseases on the incidence of erectile dysfunction / R. Shiri, J. Koskimaki, M. Hakama et al. // Urology. – 2003. – Vol.62(6). – P.1097-1102.
10. Seyoum, V. Impotence in Ethiopian diabetic men / B. Seyoum // East. Afr. Med. J. – 1998. – Vol.75(4). – P.208-210.
11. Comorbidities associated with diabetic foot complications among Asian Americans in southern California / PY Han, R. Ezquerro, KM Pan et al. // J Am Podiatr Med Assoc. – 2003. – Vol.93(1). – P.37-41.
12. Diabetic autonomic neuropathy / AI Vinik, RE Maser, BD Mitchell, R. Freeman // Diabetes Care. – 2003. – Vol.26(5). – P.1553-1579.
13. Rozhivanov, R.V. Erectile dysfunction in patients with diabetes mellitus: screening, structure, prognostic significance: Author's abstract. dis. Ph.D. honey. Sci. – 2005.
14. Nitric oxide as a mediator of relaxation of the corpus cavernosum in response to nonadrenergic, noncholinergic neurotransmission / J. Rajfer, WJ Aronson, PA Bush et al. // N Engl J Med. – 1992. – Vol.326(2). – P.90-94.
15. Nusbaum, MR Erectile dysfunction: prevalence, etiology, and major risk factors / MR Nusbaum // J Am Osteopath Assoc. – 2002. – Vol.102(12), Sup.4. – P.1-6.
16. Protein and gene expression of nitric oxide synthase isoforms I and III in the rat penile shaft / CM Gonzalez, RE Brannigan, T. Bervig et al. // J Androl. – 2001. – Vol.22. – P.54-61.
17. Sullivan, ME Vascular risk factors and erectile dysfunction / ME Sullivan, SR Keoghane, MA // Br J Ural Int. – 2001. – Vol.87. – P.838-845.
18. Nitricoxide and penile erection, is erectile dysfunction another manifestation of vascular disease? / ME Sullivan, CS Thompson, MR Dashwood et al. // Cardiovasc Res. – 1999. – Vol.43(3). – P.658-665.
19. Cartledge, JJ, Impairment of corpus cavernosal smooth muscle relaxation by grycosylated haemoglobin / JJ Cartledge, I. Eardley, JFB Morrison // Br J Urot Int. – 2001. – Vol.85. – P.735-741.
20. Cartledge, JJ Advanced glycation end-products are responsible for the impairment of corpus cavemosal smooth muscle relaxation seen in diabetes / JJ Cartledge, I. Eardley, JF Morrison // Br J Urol Int. – 2001. – Vol.87(4). – P.402-407.
21. Molecular and biological properties of the vascular endothelial growth factor family of proteins / N. Ferrara, K. Houck, L. Jakeman, DW Leung // Endocr Rev. – 1992. – Vol.13(1). – P.18-32.
22. Advanced glycation end products induce expression of vascular endothelial growth factor by retinal Muller cells / C. Hirata, K. Nakano, N. Nakamura et al. // Biochem Biophys Res Commun. – 1997. – Vol.236(3). – P.712-715.
23. Sarman, B. Role of endothelin-1 in diabetes mellitus / B. Sarman, M. Toth, A. Somogyi // Diabetes Metab Rev - 1998. - Vol. 14 (2). – P.171-175.
24. Retter, AS Carnitine and its role in cardiovascular disease. / AS Retter // Heart Dis. – 1999. – Vol.1(12). P.108113.
25. Changes in the VIPergic, cholinergic and adrenergic innervation of human penile tissue in diabetic and non-diabetic impotent males / J. Lincoln, R. Crowe, PF Blacklay et al. // J Urol. – 1987. – Vol.137(5). – P.1053-1059.
26. Neuropathy is a major contributing factor to diabetic erectile dysfunction / MJ Hecht, B. Neundorfer, F. Kiesewetter F, MJ Hilz // Neural Res. – 2001. – Vol.23(6). – P.651-654.
27. Harati, Y. Diabetes and the nervous system / Y. Harati // Endocrinol Metab Clin North Am. – 1996. – Vol.25(2). – P.325-359.
28. Aetiopathogenesis and management of impotence in diabetic males: four years experience from a combined clinic / A. Veves, L. Webster, TF Chen et al. // Diabet Med. – 1995. – Vol.12(1). – P.77-82.
29. Hakim, LS, Goldshtein I. Diabetic sexual dysfunction / LS Hakim, I. Goldshtein // Endocrinol. Metab. Clin. N. Am. – 1996. – Vol.25(2) – P.379-400.
30. Stevens, M. J. Diabetic peripheral neuropathy. Current therapy of diabetes mellitus / MJ Stevens, EL Feldman, DA Greene // Eds. R.A. Defronzo. – St. Louis: Mosby. – 1998. – P.160-165.
31. Balabolkin, M.I. Pathogenesis of angiopathy in diabetes mellitus / M.I. Balabolkin, E.M. Klebanova, V.M. Kreminskaya // Diabetes mellitus. – 1999. – No. 1. – P.2-9.
32. Kalinchenko, S.Yu. Neurogenic disorders of sexual function in men suffering from diabetes mellitus / S.Yu. Kalinchenko, R.V. Rozhivanov // Doctor. – 2006. – No. 1. – P.48-51.
33. Kurbatov, D.G. Erectile dysfunction in patients with diabetes mellitus / D.G. Kurbatov, R.V. Rozhivanov, D.V. Priymak // Russian Medical Journal – 2009. – No. 17(25). – P.1672-1676.
34. Rossi, P. Comparison between plasma concentrations of testosterone, nitric oxide and endothelin 1-2 in penile and brachial venous blood: preliminary results in men with psychogenic impotence / P. Rossi, F. Menchini Fabris, I. Fiorini et al. // Biomed. Pharmacother. – 1998. – Vol.52(7-8). – P.308-310.
35. Schirar, A. Localization of androgen receptor in nitric oxide synthase and vasoactive intestinal peptide containing neurons of the major pelvic ganglion innervating the rat penis / A. Schirar, C. Chang, JP Rousseau // J. Neuroendocrinol. – 1997. – Vol.9(2). P.141-150.
36. Hormones and nocturnal penile tumescence in healthy aging men / RC Schiavi, D. White, J. Mandeli, P. Schreiner-Engel // Arch. Sex. Behav. – 1993. – Vol.22(3). – P.207-215.
37. Erectile dysfunction and lower androgenicity in type 1 diabetic patients / O. Alexopoulou, J. Jamart, D. Maiter et al. // Diabetes Metab. – 2001. Vol.27(3). – P.329-336.
38. Cunningham, MJ Leptin's actions on the reproductive axis: perspectives and mechanisms / MJ Cunningham, DK Clifton, RA Steiner // Biol. Reprod. – 1999. – Vol.60. – P.216-222.
39. Laurent, O.B. Modern methods of diagnosis and treatment of erectile dysfunction / O.B. Laurent, P.A. Shcheplev, S.N. Nesterov, S.A. Kuharkin // Russian Medical Journal. – 2000. – No. 8(3). – P.130-134.
40. Dedov, I.I. Federal target program "Diabetes mellitus". / I.I. Dedov, M.V. Shestakova, M.A. Maksimova //Methodological recommendations. 2002.
41. Tiktinsky, O.L. Andrology. / O.L. Tiktinsky, V.V. Mikhailichenko // Media Press. – 1999.
42. Physical neurological examination as a screening method for diagnosing neurogenic erectile dysfunction in patients with diabetes mellitus / R.V. Rozhivanov, O.N. Bondarenko, O.V. Udovichenko and others // Doctor. – 2005. – No. 5. – P.29-30.
43. Sexual dysfunction in men with diabetes mellitus. / Ed. M.I. Kogan // Moscow. – 2005.
44. Mazo, E.B. Comparative assessment of electromyography indicators of the penis and microscopy data of cavernous tissue in patients with erectile dysfunction in the diagnosis of cavernous innervation / E.B. Mazo, D.G. Dmitriev, D.Yu. Khudoley // Andrology and genital surgery. – 2000. – No. 1. P.55-56.
45. Aggour, A. Evaluation of the role of corpus cavernosum electromyography as a noninvasive diagnostic tool in male erectile dysfunction / A. Aggour, H. Mostafa, H. El-Shawaf // Int Urol Nephrol. – 1998. – No. 30(1). – P.75-79.
46. Ultrasound diagnosis of diseases of the external genital organs in men / A.R. Zubarev, M.D. Mitkova, M.V. Koryakin, V.V. Mitkov // Moscow. – 1999.
47. Kurbatov, D.G. Possibilities of treating genital neuropathy with phosphodiesterase type 5 inhibitors in patients with diabetes mellitus / D.G. Kurbatov, R.V. Rozhivanov // Urology. – 2009. – No. 5. – P.48-49.
48. Rafalsky, V.V. Approaches to the rational choice of phosphodiesterase type 5 inhibitors / V.V. Rafalsky // Pharmateka. – 2004. – No. 19(20). – P.1-8.
49. Vardenafil Diabetes Study Group. Vardenafil, a new phosphodiesterase type 5 inhibitor, in the treatment of erectile dysfunction in men with diabetes: a multicenter, double-blind, placebo-controlled, fixed-dose study / I. Goldstein, J. M. Young, J. Fischer et al. // Diabetes Care. – 2003. – Vol.26. – P.777-783.
50. Impact of diabetes mellitus on the severity of erectile dysfunction and response to treatment: analysis of data from tadalafil clinical trials / V. Fonseca, A. Seftel, J. Denne, P. Fredlund // Diabetologia. – 2004. – Vol.47. – P.1914-1923.
51. Giuliano, F. Tadalafil: a novel treatment for erectile dysfunction / F. Giuliano, L. Varfnese // Eur. Heart. J. Suppl. – 2002. – Vol.4(sup.H) – P.24-31.
52. Effects of Tadalafil on erectile dysfunction in men with diabetes / I. Sáenz de Tejada, G. Anglin, JR Knight, JT Emmick // Diabet. Care. – 2002. – Vol.25. – P.2159-2164.
53. Combination therapy of Tadalafil & Testosterone in hypogonadal nonresponders / A. Yassin, HE Diede, F. Saad, A. Traish // Int. J. Impot. Res. – 2003. – Vol.15(Sup.6). – P.27.
54. Rozhivanov, R.V. Features of the treatment of erectile dysfunction in patients with hypogonadism / R.V. Rozhivanov, D.G. Kurbatov // Doctor. – 2009. – No. 3. – P.65-69.
55. Features of correction of sexual dysfunction in men with diabetes / R.V. Rozhivanov, A.E. Lepetukhin, S.A. Dubsky, D.G. Kurbatov // Diabetes mellitus. – 2010. – No. 3. – P.30-31.
56. Hackett, G. PDE5 inhibitors in diabetic peripheral neuropathy / G. Hackett // Int J Clin Pract. – 2006. – Vol.60. P.1123-1126.
57. Ziegler, D. Clinical aspects, diagnosis and therapy of diabetic neuropathy / D. Ziegler // Ther Umsch. – 1996. – Vol.53(12). – P.948-957.
58. Alpha lipoic acid: a new treatment for neuropathic pain in patients with diabetes? / GS Mijnhout, A. Alkhalaf, N. Kleefstra, HJG Bilo // The Netherlands Journal of Medicine. – 2010. – Vol.64. – P.158-162.
Magazine
Bulletin of Urology No. 2/2014
Comments
To post comments you must log in or register