Kidneys are paired bean-shaped organs that perform regulatory functions in relation to chemical homeostasis in the human body and belong to the urinary system. The kidneys remove excess organic molecules (such as glucose molecules) from the blood and play an important role in the process of urine formation by removing organic waste, including urea, from the body.
Performing a homeostatic function, the kidneys play an important role in the urinary system, regulating the acid-base balance and the amount of electrolytes in the human body. By maintaining the body's salt and water balance, the kidneys regulate blood pressure. The kidneys are a natural filter for the blood, removing soluble waste and excess water and sending them to the bladder.
During urine formation, the kidneys excrete waste products such as urea and ammonium and are responsible for the reabsorption of water, amino acids and glucose.
It should also be noted that the kidneys are involved in the formation of certain hormones, including: erythropoietin, calcitriol. This organ also secretes the enzyme renin, which acts in a negative feedback loop on the kidneys, playing a role in regulating blood pressure.
Kidney structure
The kidneys are located in the posterior part of the abdominal cavity in the retroperitoneal space, behind the parietal layer of the peritoneum. The kidneys are attached to the posterior abdominal wall in the projection of the 11th and 12th thoracic vertebrae, as well as the 1st and 2nd lumbar vertebrae. In a normal person, the right kidney is located slightly lower than the left kidney. This is due to the fact that the liver is located above the right kidney. The upper parts of the kidneys are partially covered by the 11th and 12th ribs. The kidneys are surrounded by two layers of adipose tissue (the perinephric layer and the perirenal layer of fat), as well as the renal fascia. The length of the bud ranges from 115 to 125 mm, width 50-60 mm and thickness 30-40 mm. The left kidney is slightly larger than the right, each weighing from 120 to 200 g. In women, the kidneys weigh on average 10% less than in men. Each kidney secretes urine into a ureter, which has a paired structure and drains into the bladder.
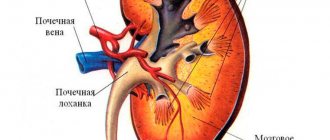
Each bud is bean-shaped and has convex and concave surfaces. The concave surface is the renal hilum (renal scar), where connections to the renal artery, renal vein and ureter are located. Each kidney is surrounded by tough fibrous tissue, the renal capsule, which is surrounded by a perirenal fat layer, renal fascia, and a perinephric fat layer. The front part of these tissues borders the peritoneum, and the rear part borders the transversal fascia. The upper part of the right kidney is adjacent to the liver, and the upper part of the left kidney is adjacent to the spleen.
The kidney consists of two main structural layers. The superficial layer is called the renal cortex (cortex), and the inner layer of the kidneys is called the medulla . Macroscopically, these substances represent from 8 to 18 cone-shaped renal petals, consisting of cells of the renal cortex surrounding part of the medulla. Between the renal pyramids there are renal projections called renal columns. Nephrons , which are the urine-producing structures of the kidneys, fill the cortex and border with the renal medulla. Moreover, 85% of nephrons are located in the renal cortex. Nephron tubules form loop-like structures that penetrate the renal medulla. Some nephrons perform initial filtration in the renal calculus, located in the cortex. Each human kidney contains approximately 1,000,000 nephrons. Part of the renal cortex and medulla are renal tubules, which connect into a single collection channel.
From the head or papilla of each pyramid, urine flows into small calyces from which the urine then flows into large calyces, after which from the large calyces it flows into the renal pelvis and then into the ureter. At the renal hilum, the renal vein and ureter have their exit from the kidneys, and the renal artery has their entrance. The right and left ureters then empty into the bladder.
Kidney number abnormalities
Quantity abnormalities are quite common and account for about 30% of all renal defects.
Aplasia (agenesis)
kidneys are the complete absence of a kidney and renal vessels. This anomaly occurs when the metanephros duct does not grow to the metanephrogenic blastema. The frequency of this defect is 0.05-0.1%, in women 3 times less often than in men. In this case, the ureter may be normal, shortened or completely absent. The complete absence of the ureter is combined in men with the absence of the vas deferens, cystic changes in the seminal vesicle, hypoplasia or absence of a testicle on the same side, hypospadias, which is associated with the characteristics of embryonic morphogenesis. In women, renal aplasia can be combined with a one- or two-horned uterus, absence or hypoplasia of the uterus and absence or underdevelopment of the vagina (Rokitansky-Kuster-Hauser syndrome). The absence of the ipsilateral adrenal gland accompanies renal agenesis in 8-10% of cases. Compensatory hypertrophy of the contralateral kidney is almost always observed with renal aplasia. Bilateral aplasia is incompatible with life. A reliable diagnosis can only be made using X-ray renal angiography, as well as spiral or MSCT and magnetic resonance angiography. All other diagnostic methods should not be considered reliable.
Kidney duplication
- one of the most common anomalies. According to sectional statistics, it occurs in 1 case in 150 autopsies. In women it is 2 times more common. It can be either unilateral - 89%, or bilateral - 11%. Kidney duplication occurs when two foci of induction of differentiation are formed in the metanephrogenic blastema. In this case, two pyelocaliceal systems are formed, but complete separation of the blastemas does not occur, and therefore the kidney is covered with a common fibrous capsule. Each half of the doubled kidney has its own blood supply. The renal vessels can arise separately from the aorta or through a common trunk, dividing at the renal sinus or nearby. Some intrarenal arteries pass from one half to the other, which can be important when performing partial nephrectomy. The common feature of the double kidney is a fibrous capsule. Most often the upper half is underdeveloped; very rarely both halves are functionally the same or the lower half is underdeveloped. The underdeveloped half in its morphological structure resembles kidney dysplasia. The presence of parenchymal renal dysplasia in combination with urodynamic disorders, due to splitting of the ureter, creates natural preconditions for the occurrence of diseases in the abnormal kidney. Most often, when a kidney is doubled, diseases such as chronic (53.3%) and acute (19.8%) pyelonephritis, urolithiasis (30.8%), hydronephrosis of one of the halves (19.7%) occur.
Accessory (third) kidney
- one of the rarest kidney anomalies. This defect is almost always one-sided. The genesis of the origin of this defect is similar to the genesis of kidney duplication, however, too rapid differentiation leads to the complete separation of two metanephrogenic blastemas and the formation of two kidneys. The accessory kidney always has its own fibrous capsule, blood supply system, pyelocaliceal system and ureter. The ureter often opens with an additional third orifice into the bladder, below and medial to the two main orifices, but it can also merge with the ureter of the main kidney as a ureter fissus (split ureter). With the development of highly informative diagnostic methods (ultrasound, SCT, MRI), the number of observations of an additional kidney is increasing. The most common disease of the accessory third kidney is hydronephrosis. When a pathological process develops in the accessory kidney, it is usually removed.
Blood supply to the kidneys
The kidneys receive blood from the paired renal arteries, which arise from the abdominal aorta, and give blood to the paired renal veins. Even though the kidneys are small, they receive about 20% of every cardiac output. Each branch of the renal arteries enters the segmental arteries, then dividing into interlobar arteries, penetrating the renal capsules and passing through the renal columns between the renal pyramids. The interlobar arteries carry blood to the arcuate arteries passing through the border of the cortex and medulla of the kidneys. Each of the arcuate arteries supplies blood to several interlobar arteries of the kidney, which feed the afferent arterioles that supply blood to the renal glomeruli.
The medullary interstitium is the functional space in the kidneys for filters (glomeruli), which are richly penetrated by blood vessels. The interstitium absorbs fluid extracted from urine. Once filtered, the blood is directed through small networks of venules that converge into interlobular (interlobular) veins. The distribution of veins in the kidneys follows the same pattern as the distribution of arterioles. The interlobar veins supply blood to the arcuate veins and then back to the interlobar veins, which join to form the renal vein, which exits the kidney.
The renal artery enters the kidney at the level of the first lumbar vertebra just below the superior mesenteric artery. After entering the kidney, the renal artery divides into branches: the first segmental artery, which divides into 2-3 lobar arteries, then it divides into interlobar arteries, forming afferent arterioles, which form the renal glomerulus. Here the afferent arterioles leave the renal glomerulus and divide into peritubular capillaries, which drain into the interlobular and then arcuate veins, and then into the interlobar veins, which drain into the lobar vein, which opens into the segmental vein, which drains into the renal vein. Blood then moves from the renal vein to the inferior vena cava.
Kidney functions
The kidneys are involved in homeostasis throughout the body. They regulate electrolyte concentrations and acid-base balance, and also regulate blood pressure and extracellular fluid volume. These functions of the kidney are performed both independently and in interaction with other organs, mainly with the organs of the endocrine system. Endocrine hormones regulate some of the functions of the kidneys. These include renin, angiotensin 2, antidiuretic hormone, aldosterone, natriuretic peptide.
Most of the functions of the kidneys are simple filtration, reabsorption and secretion, occurring in the nephrons of the kidneys. Filtration that occurs in the renal carpuscules is the process by which cells and large proteins are filtered out of the blood, thereby producing an ultrafiltrate, which then becomes urine. The kidneys produce approximately 180 liters of filtrate per day, but produce only about 2 liters of urine. Reabsorption is the transport of molecules from the ultrafiltrate into the blood. Secretion in the kidneys involves the reverse process where molecules from the blood are transported into the urine.
The kidneys excrete various waste products that are produced by metabolizing substances into urine. Such wastes include uric acid, urea, and nitrogenous wastes of protein catabolism.
It should be noted that the organs that maintain the acid-base balance of the body include two paired organs - the lungs and the kidneys. The lungs regulate acid-base homeostasis by regulating the concentration of carbon dioxide in the blood. The role of the kidneys in regulating acid-base balance is to reduce bicarbonate from urine and release fixed acids and hydrogen ions into the urine.
Peculiarities
In origin, the pathology resembles doubling, but during division the processes are accelerated, which leads to the appearance of a third full-fledged organ. The development of cells and tissues occurs only in a one-sided manner.
The accessory kidney has a capsule formed of connective or fibrous tissue. And also the system through which blood circulation occurs. The third organ consists of the calyx of the pelvis. The proper ureter enters the bladder through the orifice or merges with the main ureter.
Typically, the development of the third kidney is accompanied by hydronephrosis (enlargement of the kidney elements due to improper outflow of urine). If the pathological process in the third kidney worsens the state of health and causes discomfort, the question of its removal is raised.
The additional kidney may not manifest itself for some time. Sometimes the patient does not suspect the deviation. During a routine examination of organs using ultrasound, the doctor immediately sees the pathology.
In other cases, people deliberately go for examination when they discover unpleasant symptoms, such as urinary incontinence. In this case, the pathology openly declares itself, which is noticeable by the malfunction of the urinary system. The ureter at the third kidney is formed with insertion into the rectum or vaginal wall. Urine output is not controlled and cannot be corrected on its own without medical assistance.
Regulation of blood pressure by the kidneys
Although the kidneys cannot directly affect the blood, they play an important role in regulating blood pressure. This occurs by controlling extracellular fluid cells, the size of which depends on plasma sodium concentration. Among the important chemical elements that make up the renin-angiotensin system, renin plays an important role. Changes in renin alter the release of hormones such as aldosterone and angiotensin 2 from this system. Each hormone acts through several mechanisms to increase renal reabsorption of sodium chloride, dilate extracellular fluid cells, and increase blood pressure. The relationship with renin levels is direct. When renin levels increase, the levels of aldosterone and angiotensin 2 increase, which, according to the above scheme, leads to an increase in blood pressure. At low renin levels the process is opposite.
Kidney diseases
Kidney diseases are divided according to the type of damage to these organs. They are diffuse (bilateral) and unilateral diseases. Diffuse kidney damage includes diseases when both kidneys are affected by the disease and the whole body suffers from this; serious disturbances in the function of both kidneys occur. Bilateral kidney damage leads to pathological changes in other human organs. Such kidney diseases include nephrosclerosis and nephritis.
Unilateral kidney diseases usually affect one kidney and often do not lead to serious impairment of their function or to pathological changes in the body. Such diseases include kidney tuberculosis, kidney stones, kidney tumor, focal nephritis. With focal nephritis, only certain areas of the kidney are affected, while other areas function normally and the kidney copes with its functions.
Stones in the kidneys
Kidney stones (kidney deposits) are hard, crystal-like formations in the kidneys that form from crystals in the urine. Small kidney stones usually leave the kidneys in the urine and do not cause painful symptoms, but sometimes the crystals can be deposited for a long time and the stones reach such a size that they make themselves known or are passed with very severe pain. If a kidney stone reaches a diameter of more than 3 mm, it can cause blockage of the ureter. This leads to severe pain that spreads from the lower back to the groin area and lasts in attacks of 20-60 minutes. Blockage of the ureter causes decreased kidney function and enlargement of the organ. Symptoms such as nausea, vomiting, fever, blood or pus in the urine, and pain when urinating are also often present.
The diagnosis of kidney stones is made based on the results of urine tests, ultrasound and x-rays of the kidneys. Almost 80% of kidney stones occur in men. Kidney stones are classified according to their location and composition.
The main symptoms indicating the presence of kidney stones are pain below the chest level and slightly above the pelvic level. The difference between the symptoms of the presence of stones that block the ureter or are located in the renal pelvis is severe periodic pain radiating to the groin or inner thigh. This is a special, distinctive type of pain that is one of the most severe types of pain.
The main causes of kidney stones are low fluid intake, high levels of animal protein intake, refined sugar, sodium, and fructose. Apple and grapefruit juices also increase the risk of kidney stones. Kidney stones are caused by Crohn's disease. This is due to the peculiarities of magnesium absorption in this disease and, with hyperoxaluria.
Calcium is the most common element that forms kidney stones. Studies conducted in the 90s of the 20th Century showed that the risk group for kidney stones includes people who consume dietary supplements high in calcium. Thus, according to these studies, postmenopausal women who consumed an additional 1000 mg of calcium per day and vitamin D for 7 years had a 17% higher risk of developing kidney stones than ordinary people. At the same time, consuming additional dietary calcium, on the contrary, not only does not cause the formation of kidney stones, but, on the contrary, may reduce the risk of their development.
Low levels of magnesium intake also cause kidney stones.
Excess sulfur amino acids from animal fats increase the risk of developing kidney stones, as they further acidify the urine.
Taking vitamin D may also cause kidney stones because it increases intestinal absorption of calcium.
Frequent alcohol abuse also provokes the formation of kidney stones, as it leads to a decrease in fluid levels in the body (frequent dehydration occurs).
Kidney tumor
Almost 90% of kidney tumors are renal cell carcinoma. Such tumors are called hypernephroma, renal adenocarcinoma, clear cell tumor. Wilms tumor and sarcoma are much less common. People at risk for kidney cancer include people with acquired kidney cysts, horseshoe kidneys, and Hippel-Lindau disease. It is also believed that kidney cancer is caused by certain carcinogens in aniline dyes.
Nephritis
Diffuse nephritis is characterized by inflammation of the kidneys, when the parenchyma of both kidneys is drawn into the inflammatory process. Focal nephritis affects areas of one or two kidneys, but inflammation occurs only in these small areas, while the rest of the kidneys function normally. Nephritis can be acute or chronic. In acute nephritis, inflammation usually occurs in the renal glomeruli, and capillaries and small arteries are damaged. Most often, the main cause of acute nephritis is infection with streptococcus. This is why acute nephritis occurs after tonsillitis, scarlet fever and other respiratory diseases. Hypothermia (cold) can also cause acute nephritis.
Diagnostics
The diagnosis of a double kidney in a child can cause parents to panic. But in most cases, the pathology does not manifest itself and does not pose a significant threat to the child’s health. A large number of patients live with a third kidney for many years without complications.
There are other cases where an accessory organ becomes a serious cause of disorders in the urinary system. Complications will need to be treated, and if necessary, the kidney will be removed.
What diseases can be diagnosed with the third kidney:
- inflammation of the renal pelvis (pyelonephritis);
- nephroptosis (prolapse of the main kidney);
- various degrees of nephrosis (from minor tissue damage to a necrotic state);
- constant leakage of urine (with abnormal insertion of the ureter);
- polycystic disease (formation of numerous cysts);
- kidney tuberculosis (damage to the cortex and subsequent tissue decay);
- formation of stones in the kidneys (urolithiasis).
Unfortunately, inflammatory diseases do not spare even very young children. One of the common diseases found in children under 1 year of age is pyelonephritis. You can learn about the symptoms and causes of the development of this disease in infants.
Finding the third kidney is not difficult. It is visible during standard instrumental studies. In-depth methods help to assess its condition more fully.
Applicable:
- palpation;
- ultrasonography;
- urine and blood analysis;
- X-ray.
Thanks to scintigraphy, the specialist receives extensive information about all segments of the third kidney and its functioning. During diagnosis, it is determined whether there is a negative effect from the accessory organ. If the study confirms the normal condition and harmless functioning of the organ, there is no need for its treatment. In case of pathology in a child, constant monitoring of the condition of the tissues is recommended.