Best's Dystrophy Clinic
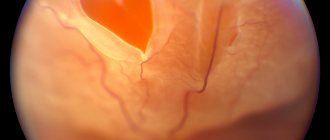
In the fundus of the eye, in the macular area, round or oval yellowish lesions (cysts) with a reddish tint are formed, which resemble egg yolk, ranging in size from 1/2 to 4 times the diameter of the optic disc. The process ends with the formation of an atrophic focus (scar) in the macula with or without subretinal neovascularization. The disease is usually detected by chance. Patients complain of blurred vision, difficulty reading texts with small print, and metamorphopsia. Visual acuity depends on the stage of the disease and can be quite high for a long time, significantly decreasing when an atrophic focus forms in the macula. Also characteristic symptoms are central scotoma and impaired color vision.
Best's disease
The first changes in the fundus of the eye with Best's disease occur at the age of 2-5 years, but no subjective symptoms are observed. Therefore, the disease is diagnosed either based on the results of a random medical examination, or at a later age, after the development of the first visual impairments. In general, Best's disease is characterized by a certain stage.
The zero stage of Best's disease is diagnosed very rarely, since there are not even minor changes in the area of the macula. Only a decrease in the foveal reflex and changes in electrooculography are observed. When studying the latter, a decrease in the Arden coefficient is revealed. Sometimes such manifestations are recorded in adults without further development of the clinical picture of Best's disease - this is considered a sign of carriage of the BEST1 gene mutation.
During the first stage, subjective symptoms are still not expressed, only in some cases there is a slight decrease in visual acuity. The fundus reveals several yellowish dots in the macular region of the retina. During the second stage, the dots grow to a size comparable to the diameter of the optic nerve head and are similar in appearance to egg yolk. Visual acuity impairments at this stage of Best's disease do not correspond to the ophthalmological picture and are insignificant - it remains at the level of 0.6-0.9. At the third stage of Best's disease, vitelliform cysts rupture, which leads to a sharp decrease in visual acuity. Also common complaints at this stage are blurred vision and difficulty reading small text. The fourth stage is characterized by the resorption of cyst rupture products and the formation of a scar in their place. Visual acuity in different patients at this stage ranges from 0.02 to 0.7, in addition, relative central scotoma and pseudohypopyon occur. The boundaries of the visual field, as a rule, do not change, and normal color perception is maintained.
The duration of each stage in different patients can vary widely. Additionally, in some cases, Best's disease may develop more quickly, so some stages may not be diagnosed. Changes in the fundus of both eyes are most often asymmetrical. As a rule, complete blindness does not occur; one of the complications of Best's disease may be the formation of a subretinal neovascular membrane, which significantly reduces visual acuity. In addition, with age, choriodal sclerosis may develop at the site of scars after vitelliform cysts.
Treatment methods for retinal dystrophy
There is no pathogenetically based treatment for hereditary macular degeneration. Wearing sunglasses is recommended to prevent light from damaging the retina. When a subretinal neovascular membrane is formed in West dystrophy, laser photocoagulation can be performed.
For each person with dystrophy, individual methods and medications must be chosen. The ophthalmologist must take into account the stage of the disease, the prevalence of dystrophy and the rate of its progression. At the very beginning, conservative methods are used, but it is not always possible to stop the process with medications.
In the case of dystrophy, it is impossible to treat with one drug. To stop destructive processes, a complex effect is necessary: vasoconstrictors, angioprotectors, diuretics, glucocorticosteroids and others. The chosen course should be repeated several times a year.
What drugs help with retinal dystrophy:
- Angioprotectors, vasodilators (No-Shpa, Ascorutin, Papaverine, Complamin). Drugs from these groups help strengthen vascular walls and expand the lumen even in the smallest vessels. It is not recommended to use medications without an ophthalmologist's prescription, since it is necessary to accurately calculate the dosage in accordance with the clinical picture.
- Antiplatelet agents (Aspirin, Ticlopidine, Clopidogrel). Antiplatelet agents are intended to normalize blood clotting in order to prevent blockage.
- Polypeptides (Cortexin, Retinalamin). These products are produced from cattle biomaterials. They help reduce the destruction of the retinal pigment epithelium, activate fibrinolysis and have an immunomodulatory effect.
- Maintaining microcirculation (Pentoxifylline). With dystrophy, it is necessary to improve blood microcirculation in the vessels so that all structures of the eye receive enough nutrients. Pentoxifylline is intended for eye injection.
- Intravitreal drugs (Avastin, Lucentis, Eylea). VEGF blockers suppress the proliferation of abnormal blood vessels and prevent pathological changes in the vascular system.
- Eye drops (Emoxipin, Taufon, Oftan-Katachrome). Drops help improve metabolism and regeneration of damaged tissues. This is a good prevention of cataracts and glaucoma.
- Vitamins. In addition to the main treatment, medications with vitamins B and C are prescribed.
- Medicines to lower cholesterol levels.
Medication treatment is often combined with physiotherapy and surgery. The effectiveness of physiotherapy for dystrophic changes has not been proven, but in practice photostimulation or laser stimulation, electrophoresis, blood irradiation, and magnetic therapy are used.
In dystrophic processes, the administration of anti-VEGF drugs is indicated. These procedures are performed only by specialists prescribed by an ophthalmologist. Anti-VEGF drugs are injected into the vitreous to maximize the effect on the center of the retina. A course of 8-10 injections over 2-3 years helps slow down pathological changes. Penetrating into tissues, the components of the drug inhibit the activity of the protein. Under such conditions, the growth of new vessels (angiogenesis) stops, they die and disintegrate.
Controlling angionesis makes it possible to eliminate swelling, stabilize vision and prevent severe damage to the macula. In 30% of people with the wet form, vision improved to an acceptable level after anti-VEGF therapy. Usually the drugs Ilia or Lucentis are used. In recent years, Avastin is often prescribed for retinal dystrophy, which was previously used only to eliminate cancerous tumors.
The help of surgeons is indicated in severe cases of dystrophy, when there is a serious threat to vision. There are several effective methods for treating degenerative processes surgically, but laser coagulation is recognized as the fastest and most effective.
Methods of surgical treatment of retinal dystrophy:
- Laser coagulation. The method does not require opening the eye; all manipulations are carried out contactlessly. The risk of infection and postoperative complications is eliminated. Laser surgery is indicated even for pregnant women and girls.
- Revascularization and vasoreconstruction. Treatment involves restoring blood vessels using various microsurgical methods and improving the blood supply to the retina by cutting the arteries.
- Vitrectomy. In case of lateral dystrophy, the vitreous body may be removed and replaced with a special material to prevent or treat retinal detachment. The replacement does not affect the functioning of the eyeball, since biologically compatible materials are used.
Treatment of retinal dystrophy with laser is fast, low-traumatic and bloodless. The doctor uses laser pinpoint radiation to target areas of pathology. Damage to healthy tissue is completely excluded, and the risk of side effects and complications is minimal. The transpupillary method and focal coagulation are recognized as the most effective.
Transpupillary treatment involves using a weak, wide-area laser. A small amount of energy prevents the formation of coagulants, but has a positive effect on the functioning of the fundus. Phagocytes are activated, blood flow improves, and the antioxidant properties of the retina increase.
Focal coagulation is recommended for patients with peripheral dystrophy when the macula is almost unaffected. The doctor creates point coagulants on the retina to minimize the risk of detachment. After treatment, patients need to take angiogenesis inhibitors to prevent the growth of abnormal blood vessels.
Retinal dystrophy is a common and dangerous disease. It is usually diagnosed in older people, but young people should also monitor their health, take preventive measures and visit an ophthalmologist twice a year.
There is no specific treatment for Best's disease; therefore, maintenance therapy is used, which can significantly slow down the progression of the pathology. This includes the administration of vitamins A and E, vasodilators and agents that improve retinal trophism - meldonium, methylethylpyridinol, ethylmethylhydroxypyridine succinate. This inhibits the development and subsequent rupture of vitelliform cysts, allowing satisfactory visual acuity to be maintained for a long time. In cases where Best's disease is complicated by the formation of a subretinal neovascular membrane, laser correction is indicated.
The prognosis for Best's disease is usually conditionally favorable. Complete loss of vision occurs in very rare cases; usually everything is limited to a decrease in visual acuity and a relative central scotoma. Peripheral and twilight vision is not affected; patients subsequently only have difficulty working with small fonts and small details. In adult vitelliform dystrophy, visual impairment is even less pronounced; in some cases, patients have no complaints at all, and the presence of the disease is determined only by ophthalmological and genetic studies.
Symptoms of retinal dystrophy
For retinal pigmentary degeneration
the pigment epithelium and photoreceptor cells are affected. The first signs appear in early childhood. Characteristic specific symptoms: pigmented lesions (bone bodies), atrophic optic disc and narrowed arterioles.
With Leber's congenital amaurosis
Blindness occurs from birth or children lose vision before age 10. Features: lack of central vision, nystagmus, keratoconus, strabismus, etc. Various degenerative foci are identified throughout the fundus (white and pigmented salt and pepper type, bone bodies), the optic disc is pale, the vessels are narrowed.
X-chromosomal juvenile retinoschisis
refers to hereditary vitreochorioretinal dystrophies. In this case, retinal dissection occurs, cysts form on the periphery, into which hemorrhages can occur. In the vitreous body there is hemophthalmos, strands that can lead to retinal detachment.
Wagner's disease
manifested by myopia, reshinoschisis, pigmentary dystrophy and preretinal membranes with a transparent vitreous body.
Goldman-Favre disease
– hereditary dystrophy has a progressive course, the main manifestations of which are bone bodies, retinoschisis and vitreous degeneration. Stargardt's disease affects the macular area. A characteristic sign in the fundus is a “bull’s eye” in the central zone, that is, a dark area with a light ring surrounded by rounded hyperemia. Symptoms include decreased visual acuity by age 20, impaired color vision and spatial contrast sensitivity.
Best's vitelline dystrophy
– a yellowish focus forms in the macular area, resembling the yolk of an egg. At the age of approximately 10-15 years, decreased vision, distortion of the shape of objects, and “fog” before the eyes appear. Both eyes are affected to varying degrees.
Age-related (involutional, senile) central retinal dystrophy
– one of the most common causes of decreased vision in people over 50 years of age with a hereditary predisposition.
There are 2 forms:
Non-exudative – characterized by pigment redistribution, drusen, and areas of retinal dystrophy. The lesions can merge, resembling a “geographic map” picture. Drusen are located under the pigment epithelium and have a yellowish-white color; they may proliferate into the vitreous body. There are soft (with unclear boundaries), hard (with clear boundaries) and calcified. The course of the non-exudative form is benign, develops slowly
Exudative – in its development it goes through several stages: exudative detachment of the pigment epithelium, exudative detachment of the neuroepithelium, neovascularization, exudative-hemorrhagic detachment, reparative stage. Quickly leads to blindness.
Risk factors for age-related macular degeneration: blue eyes and white skin, diet low in vitamins and minerals, high cholesterol, smoking, hypertension, hypermetropia, cataracts, previous eye surgery.
The main complaints of patients with retinal dystrophies
: decreased visual acuity often in both eyes, narrowing of the visual field or the appearance of scotomas, nyctalopia (poor vision in the dark), metamorphopsia, impaired color vision.
If any of the above symptoms appear, you must contact a specialist who will make the correct diagnosis and prescribe treatment.
Best's disease - causes, symptoms and treatment
Retinal dystrophy may be congenital. If inheritance is dominant, dystrophy manifests itself at an early age and progresses rapidly. Dystrophy, inherited recessively, makes itself felt at a later age (up to 30 years). The congenital form combines pigmentary dystrophy (deterioration of vision at dusk) and Best syndrome (damage to the receptors of the macula). This form of the disease is irreversible.
The acquired type of dystrophy is usually detected in people over 60 years of age, and is often combined with clouding of the lens (cataract). In young patients, dystrophy begins for a variety of reasons, but the main percentage consists of people with vascular diseases and refractive disorders of vision.
Causes of acquired retinal dystrophy:
- active tissue scarring due to vascular dysfunction;
- improper functioning of the immune system;
- unbalanced diet, low-quality or dangerous products, non-compliance with the regime;
- bad habits (smoking and drinking);
- complicated viral infections without proper therapy;
- chronic systemic diseases (diabetes mellitus, cardiovascular pathologies, hypertension, endocrine disruptions);
- metabolic disorders, obesity;
- poor-quality surgical treatment of the visual organs.
An early warning symptom is weakening of twilight vision. This condition is also called night blindness or night blindness. It becomes difficult to adapt to insufficient lighting, the boundaries of the field of vision are narrowed and lateral vision is impaired. Gradually, due to trophic disturbances, cataracts and retinal detachment join the dystrophic processes, and sometimes intraocular pressure increases.
Signs of retinal dystrophy:
- no adequate color perception;
- distortion of visible objects;
- blurred vision, feeling of a veil;
- disturbance of central or lateral vision;
- bright flashes, flies in the field of view;
- incorrect perception of moving and static objects;
- feeling of insufficient lighting.
Best's disease is called childhood macular degeneration. This pathology is the most rare retinal dystrophy in the macula area and has the appearance of a delimited yellowish circle. The appearance of the degeneration zone has become the reason for another name for this pathology - vitelline degeneration.
Also, such degeneration is usually called childhood degeneration, since it is detected only in children 5–15 years old.
According to the method of inheritance, Best's dystrophy is classified as an autosomal dominant type. A gene located on the long arm of chromosome number eleven is directly related to the development of the disease.
It is impossible to identify the disease in advance; it is asymptomatic. In rare cases, patients may complain of problems reading small print, sometimes blurred vision, and metamorphopsia. Especially often, such a pathology is discovered by chance during the next ophthalmological examination.
MORE ABOUT: DEFISLEZ® (hypromellose) - eye drops
Signs of the disease
Best's dystrophy occurs due to the accumulation of transudate under the pigment epithelium. Such an accumulation can sometimes reach three times the diameter of the optic nerve head and lead to ophthalmological changes in the macula area of the eye. Depending on the intensity of such changes, it is customary to distinguish certain stages of the development of the disease:
- Previtellifoma stage, when small yellow spots and minimal pigmentation disturbance are found in the macula;
- Vitelliform stage with a vitelliform cyst in the macula;
- The stage of cyst rupture and resorption of its contents;
- Stage of fibroglial scar formation.
In its development, Best's disease does not always strictly go through all of the above stages; sometimes slight variations in the manifestations of the disease are possible. Changes, as a rule, are bilateral, asymmetrical. Visual acuity decreases only by the 3rd stage, remaining in the range from 0.02 to 1.0D.
Over time, degeneration of the external components of photoreceptors is possible. Without proper adequate treatment, Best's disease can be complicated by the formation of a subretinal membrane and subretinal hemorrhages.
In rare cases, this condition can lead to retinal detachment, as well as choroidal sclerosis.
Diagnosis of childhood macular degeneration is based on the results of ophthalmoscopy, electroretinography and electrooculography readings. Fluorescein angiography is often used to confirm it. In complex situations, examination of the patient's family members may be necessary to assist in diagnosis.
In the case of a clearly defined yolk cyst, it is not difficult to make a diagnosis, but with unclear boundaries of the cyst and resorption of its contents, there is a need for differential diagnosis. It is necessary to differentiate Best's disease from myopic maculitis, Stargardt's disease, serous macular edema, cystic degeneration of the macular zone, and choroiditis.
Treatment of the disease
There is currently no effective and efficient treatment for Best's disease. Since the disease is usually characterized by the absence of symptoms that bother the patient, doctors, as a rule, do not take any special measures. In the case of the formation of a subretinal membrane, which can cause minor visual defects, laser coagulation of the retina is sometimes performed.
Compared with Best's disease, macular degeneration does not progress in adults and is associated with smaller lesions.
In the medical department, everyone can undergo examination using the most modern diagnostic equipment, and based on the results, receive advice from a highly qualified specialist. We are open seven days a week and open daily from 9am to 9pm.
Experienced refractive surgeons, detailed diagnostics and examination, as well as the extensive professional experience of our specialists allow us to ensure the most favorable result for the patient.
You can find out the cost of a particular procedure or make an appointment at the Moscow Eye Clinic by calling multi-line phone 8 (daily from 9:00 to 21:00, free for mobile phones and regions of the Russian Federation) or using the online registration form.
specialist of the “Moscow Eye Clinic” Tsvetkov Sergey Alexandrovich
: June 16, 2016
The cause of retinal dystrophy, which occurs in Best's disease, is a mutation of the BEST1 gene, localized on chromosome 11. It encodes the protein bestrophin, which belongs to the class of anion channels of the retinal pigment epithelium. The pathogenesis of disorders in Best's disease has not been thoroughly studied - it has been found that with this pathology there is a slow destruction of the pigment epithelium in the area of the macula, and the properties of Bruch's membrane change.
As a result of this, capillaries grow into the subretinal space, and granules of a substance that is similar in its biochemical properties to lipofuscin accumulate in the retina. Macroscopically, with Best's disease, pigment disorders slowly increase in the area of the macula, then a cyst appears, which blocks the flow of light to most of the photoreceptors of the macular area. Then the cyst ruptures, its contents are resorbed, and a scar is formed in its place, which is the cause of persistent visual impairment.
The mechanism of inheritance of BEST1 gene mutations is autosomal dominant with a fairly high penetrance. In addition to Best's disease, disturbances in the structure of this gene can cause some other forms of retinal pigmentary degeneration, bestrophinopathy, and adult vitelliform dystrophy. The latter is very similar in its course to Best's disease, but unlike it, it develops not in childhood, but in adulthood.
Causes of occurrence and mechanism of development
The gene code-named BEST1 is responsible for the development of Best's disease; it is located on the long arm of the eleventh chromosome. It is he who encrypts the protein bestrophin, which belongs to the class of anion channels of the pigment epithelium of the retina.
The pathogenesis has not been fully studied.
Scientists know that the disease slowly destroys the pigment epithelium in the macula and also transforms the properties of Bruch's membrane. First, pigment disorders occur, and then a cyst gradually appears and blocks the flow of light to the vast majority of photoreceptors in the macular area.
Over time, the cystic formation ruptures, and a scar appears in its place. This is what causes vision loss.
Violation of the structure of the BEST1 gene, in addition to Best's disease, can lead to the following ailments:
- bestrophinopathy;
- vitelliform dystrophy of adults;
- other types of retinal pigmentary degeneration.
Important!
Doctors have suggested that adult vitelliform dystrophy is one of the subtypes of Best syndrome.
General information
Best's disease (central pigmentary abiotrophy, Best's vitelliform dystrophy) is a genetic disease characterized by the development of cystic degenerative changes in the macula. It was first described in 1905 by F. Best, who studied identical visual impairments in eight relatives and suggested the hereditary nature of the pathology. Best's disease affects both men and women with equal frequency, the incidence is approximately 3-4:100,000. Unlike many other forms of retinal abiotrophy, Best's disease rarely leads to complete blindness, in addition, it is characterized by a long, multi-stage course. At the initial stages of the pathology, visual impairment does not develop, and there are practically no symptoms; changes in the retina are often an accidental finding during a medical examination by an ophthalmologist. Timely prescribed maintenance therapy can significantly slow down the development of Best's disease.
Diagnostics
The diagnosis of hereditary macular degeneration is made on the basis of the fundus picture, fluorescein angiography, electroretinography and electrooculography. Genetic testing of families in which hereditary macular degeneration of the retina occurs is also important.
Vitelliform macular degeneration creates a yellow fatty pigment (lipofuscin) in the cells underlying the macula. Over time, abnormal accumulation of this substance can damage cells that are critical for clear central vision. As a result, people with this disorder often lose central vision and may see blurred or distorted vision. Vitelliform macular degeneration does not affect side (peripheral) vision or the ability to see at night.
Researchers have described two forms of vitelliform macular degeneration with similar characteristics. The early onset form (known as Best's disease) usually appears in childhood; however, the timing of symptoms and the severity of vision loss can vary widely. The adult form begins later, usually in middle age, and typically causes relatively mild vision loss. These are two forms of vitelliform macular dystrophy, each with their own characteristic changes in the macula that can be detected during an eye test.
Symptoms of the disease will differ with different localization and severity of dystrophy. The diagnosis can only be confirmed through a comprehensive and comprehensive examination of not only the visual system, but also the immune system, blood vessels and nerve fibers.
Methods for diagnosing dystrophy:
- visometry (vision test using a table);
- perimetry (visual field examination);
- ophthalmoscopy (assessment of fundus structures);
- Ultrasound;
- fluorescein angiography of blood vessels;
- checking the retina and main optic nerve at the cellular level.
Coherent optical tomography remains the most informative, showing the smallest changes in the layers of the retina. Additionally, laboratory tests are prescribed to check the functioning of the immune system and overall metabolism.
Diagnosis of Best's disease is made using modern ophthalmology methods - fundus examination, electrooculography, fluorescein angiography of retinal vessels. Upon examination, depending on the stage of the disease, either yellow dots or formed vitelliform cysts concentrated in the center are revealed. After their rupture (third stage of Best's disease), the fundus picture resembles “scrambled eggs.”
One of the very first manifestations of the disease is an abnormal electrooculography pattern, which is recorded even before the first changes appear in the fundus. The pathognomonic sign of Best's disease is a decrease in the Arden coefficient or the ratio of the light peak to the light decline, which at the final stages of pathology development does not exceed 1.5. With fluorescein angiography in the first stages of the disease (before the formation of vitelliform cysts), areas of local hyperfluorescence are observed, corresponding to areas of pigment epithelium atrophy.
MORE ABOUT: Treatment of retinal tears with surgery and folk remedies
A geneticist can also perform a genetic diagnosis of Best's disease, which boils down to sequencing the sequence of the BEST1 gene in order to search for mutations. This study is quite complex, since a huge number of genes are located in this region of the 11th chromosome, mutations of many of them can also lead to hereditary ophthalmological diseases.
Retinal dystrophy during pregnancy
During pregnancy, hormonal levels change and metabolism increases. Blood circulation in all organs and tissues first increases and then decreases.
All these changes can negatively affect the retina of the eye. Women who were diagnosed with myopia, hemeralopia and other eye diseases before pregnancy are at risk.
Due to the high risk of retinal detachment, a woman needs permission from an ophthalmologist before giving birth. If a specialist forbids giving birth on your own, they resort to artificial birth, that is, a caesarean section.
During pregnancy, a woman’s entire body undergoes enormous stress, including the tissue of the eyeball. During the entire gestation of the fetus, as well as childbirth, pressure, hormonal levels, intensity of blood flow in tissues, and metabolism change. The risk of complications such as retinal dystrophy increases, and even loss of vision is possible.
If there were visual pathologies before pregnancy, then it is necessary to be observed by an ophthalmologist throughout the entire period.
Treatment of the disease
Medicine has not yet come up with an effective therapy that could cure Best's disease.
For this reason, the doctor can only prescribe treatment that is aimed at slowing the progression of the disease.
It is worth saying right away that using traditional medicine to treat such diseases is not only pointless, but also extremely dangerous. If you start taking tinctures and decoctions at your own discretion, you can provoke an acceleration of vision loss. Do not self-medicate!
The patient is prescribed vitamins A, E and B2 or riboflavin. It is better to obtain these microelements not through pharmaceutical preparations, but from food. Patients should include chicken liver, fish, carrots, wheat germ oil, sunflower seeds, broccoli and dairy products in their diet.
Vasodilators are also prescribed to improve trophism of the retina.
Such drugs include:
- ethylmethylhydroxypyridine succinate;
- meldonium;
- Meldonium.
These drugs slow down the growth and rupture of vitelliform cysts near the corpus luteum, thereby maintaining visual acuity. If the disease is complicated by a subretinal neovascular membrane, the doctor prescribes correction to the patient using a laser.
Laser coagulation is performed in extreme cases.
With its help, bleeding from blood vessels is blocked. However, this method also does not restore vision, but only slows down its loss.