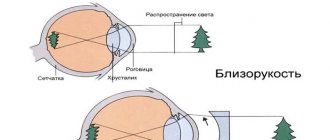
Diabetic retinopathy
Chronically high blood sugar affects the tiny blood vessels in the retina. The retina is one of the inner layers of the eye; it perceives light and converts it into impulses sent through the optic nerve to the brain. Diabetic retinopathy makes the blood vessels so fragile that microbleeds constantly occur in the retina and vision in diabetes mellitus steadily decreases.
Damage to the retina in diabetic retinopathy: microaneurysms, vascular edema and numerous hemorrhages
Diabetic retinopathy can progress in four stages:
- Mild non-proliferative stage. Small areas of balloon-like swelling of blood vessels, similar to a microaneurysm, are observed in the retina. An aneurysm is a protrusion of a pathologically altered vascular wall. In these places there is the greatest likelihood of vessel rupture and bruising.
- Moderate nonproliferative retinopathy. As the disease progresses, the blood vessels supplying the retina may swell and lose their structure. Their blood permeability is sharply reduced. This causes certain changes in the retina, namely swelling of the macula - the central zone responsible for the perception of small details. Multiple microaneurysms are detected in the fundus.
- Severe nonproliferative retinopathy. The blockage of most blood vessels, which deprives the retina of the eye of nutrition in diabetes mellitus, provokes the release of growth factor, which triggers the process of growth of new blood vessels. This is also facilitated by the formation of scars, hard exudates and hemorrhages, due to which the retinal tissue does not receive sufficient nutrition.
- Proliferative diabetic retinopathy. At this advanced stage of disease progression, growth factors secreted by the retina trigger the proliferation of new blood vessels that grow along the inner surface of the retina and into the vitreous. These newly formed blood vessels are fragile, making them more susceptible to damage and bleeding. Scar tissue forms in places where blood accumulates; it is quite rigid and therefore drags the retina along with it when moving. Thus, it separates from the choroid - tractional detachment of the retina.
The proliferative stage has four degrees of severity depending on the volume of connective tissue formations:
- I - fibrous changes in one of the zones of vascular accumulations;
- II - connective tissue changes in the optic nerve head;
- III - a combination of fibrosis of vascular clusters and the optic nerve head;
- IV – gliosis is widespread throughout the fundus of the eye, and sometimes extends to the vitreous body.
Note! Vision changes in diabetes mellitus in the following way: swelling of individual areas of the retina leads to compression of light-sensitive cells. As a result of their death, the patient does not have a complete image - in places of the retina where there are no light-catching cells, parts of the image fall out.
If there is an abundant accumulation of blood in the vitreous body, then the patient’s vision function is reduced literally to the distinction between light and darkness.
This is what patients with diabetic retinopathy see
The proliferation of fibrous tissue with subsequent separation of the retina causes permanent damage to the organs of vision, leading to blindness. As a rule, peripheral vision is lost first, then the “veil” spreads. The nature of the disease causes some return of vision after sleep or prolonged exposure to a horizontal position. Thus, the retina is purely physically adjacent to the vascular wall. When the body assumes a vertical position, the membrane again moves away from its place and the visual impairment returns.
Multiple retinal microbleeds appear as dark floats or flakes
If detachment is suspected, immediate surgical treatment is required, since being without blood supply for a long time, the cones and rods of the retina die and then vision cannot be restored.
Ocular manifestations of diabetes mellitus
VP Mozherencov, GL Prokofyeva, LAUsova The article is a clinical lecture for practical ophthalmologists. The author of the article describes main pathological changes of the eye in patients with diabetes mellitus. In diabetes mellitus, more often than in other endocrine diseases, various lesions of the organ of vision are observed - inflammatory processes of the eyelids and conjunctiva, xanthelasma of the eyelids, angiopathy of the bulbar conjunctiva and sclera, paresis of the oculomotor nerves, various forms of keratodystrophies, the development of cataracts, anterior uveitis, rubeosis of the iris, disorder hemo- and hydrodynamics of the eye. Most of the listed manifestations of the disease are nonspecific, and diabetes mellitus is considered a risk factor that increases their incidence and severity. Diabetic retinopathy is considered one of the most severe specific eye lesions in diabetes mellitus. As it progresses, it is complicated by recurrent intraocular hemorrhages, fibrosis of the retina and vitreous body, tractional retinal detachment, neovascular glaucoma, optic nerve atrophy and leads to irreversible blindness. Risk factors for patients with both insulin-dependent and non-insulin-dependent diabetes mellitus include hypercholesterolemia, proteinuria, arterial hypertension, excess body weight, infectious diseases, pregnancy and childbirth, intoxication (in particular, smoking), and surgical interventions on the eyeball. The most universal and significant risk factor is long-term decompensation of diabetes [6,7]. The pathogenesis of diabetic retinopathy is determined by impaired carbohydrate metabolism in diabetes mellitus. At the local level, a vicious circle is formed, including diffuse retinal hypoxia, increased anaerobic metabolism of the retina, the development of local acidosis, microangiopathy, venous stasis with the subsequent formation of areas of deep hypoxia and the development of proliferative processes. Pathogenetic treatment of diabetic retinopathy should be primarily aimed at eliminating or weakening at least one of three factors: hypoxia, acidosis and venous stasis [3]. The leading methods for diagnosing diabetic retinopathy are ophthalmoscopy and ophthalmomicroscopy with fluorescein angiography. The fundus picture of retinal lesions in diabetic patients is characterized by great polymorphism. At an early stage, uneven expansion, plethora and increased tortuosity of the retinal veins, single microaneurysms and pinpoint hemorrhages located in the central region are observed. As the process progresses, vascular obliteration, neovascularization, pinpoint and spot-shaped hemorrhages and yellowish-white waxy opacities occur, often merging with each other and forming ring-shaped figures around the optic nerve head, in the area of the macula and between the superior and inferior temporal arteries. The late stage of diabetic retinopathy, in addition to the described changes, is characterized by increased neovascularization with its spread to the optic nerve head, the appearance of extensive retinal and preretinal hemorrhages, often with a breakthrough into the vitreous body, proliferation of connective tissue in the retina and vitreous body in the form of membranes, cords and films , which leads to tractional detachment of the mesh, its ruptures, and secondary glaucoma. Diabetic proliferative foci in the cavity of the eyeball, in contrast to ordinary post-hemorrhagic cicatricial changes, can independently develop from newly formed vessels. The progression of diabetic retinopathy threatens irreversible blindness [1,2,7]. Diabetic retinopathy can also be benign. The benign nature of its course is determined by the duration of the disease (15–20 years), as well as the sequential development of all its stages. For the diagnosis of complications of diabetic retinopathy - proliferative changes in the vitreous body and tractional retinal detachment, especially in opaque environments of the eye, ultrasound is of decisive importance, with the help of which it is possible not only to identify, but also to localize structural intraocular changes, as well as to determine their nature and prevalence [ 3]. Cataracts are in second place in terms of the frequency of damage to the organ of vision in patients with diabetes mellitus. True diabetic cataracts occur more often in children and young people than in the elderly, more often in women than in men, and are usually bilateral. Unlike age-related ones, diabetic cataracts, especially in children, progress very quickly and can develop within 2–3 months, several days and even hours (during a diabetic crisis). Among the causes of blindness in diabetes mellitus, cataracts rank first. However, unlike blindness, retinopathy can be treated surgically. But in a significant number of patients, cataracts are combined with retinopathy, which does not guarantee a favorable outcome of the operation. In the diagnosis of the initial stages of diabetic cataract, in addition to the usual ophthalmological examination, biomicroscopy is of great importance, which makes it possible to identify flaky whitish opacities in the most superficial subepithelial layers of the lens, opacities under its posterior capsule, subcapsular vacuoles in the form of dark, optically empty, round or oval zones. With significant clouding of the lens, the specific features of diabetic cataracts are obscured. In patients with initial opacification of the lens, the refraction changes towards intensification, and a decrease in contrast sensitivity at medium and low spatial frequencies is determined [4,5]. Optic nerve lesions are relatively rare among other ocular manifestations of diabetes mellitus. Papillopathy, as a rule, occurs during decompensation of diabetes and is manifested by attacks of blurred vision and the appearance of scotomas. The fundus reveals swelling of the optic discs and signs of retinopathy. Diabetic anterior ischemic neuropathy is manifested by a unilateral decrease in visual acuity of varying severity, sectoral loss in the visual field, and papilledema. Its outcome is partial atrophy of the optic nerve with persistent impairment of visual functions. Posterior ischemic neuropathy is characterized by a significant decrease in vision with sectoral loss in the visual field against the background of an unchanged optic nerve head at the onset of the disease. The lesion is unilateral, the outcome is partial atrophy of the optic nerve. With retrobulbar neuritis, which occurs against the background of decompensation of diabetes, there is a bilateral decrease in vision and the appearance of central scotomas, but visual impairment is partially or completely reversible. Local or widespread neuropathy is a common cause of oculomotor disorders. In almost 25% of cases, paralysis or paresis of the oculomotor nerves is caused by diabetes mellitus. Distinctive features of lesions of the oculomotor system are their asymmetry and the presence of severe pain. They are observed mainly in elderly people and usually with decompensated diabetes. Depending on the course of diabetes, changes in intraocular pressure may occur. Its decrease often occurs against the background of the development of diabetic retinopathy. An acute drop in blood pressure, accompanied by constriction of the pupil and visual disturbances, indicates an incipient diabetic coma. An increase in intraocular pressure and the development of glaucoma, often secondary, occurs as a result of the formation of connective tissue and the proliferation of newly formed vessels in the anterior part of the eye, which is observed, in particular, with rubeosis of the iris. Secondary glaucoma is relatively common; when severe, it is difficult to treat and leads to irreversible blindness [2,4,6]. The leading factor in the prevention, stabilization and treatment of diabetic lesions of the organ of vision is rational therapy of diabetes mellitus, aimed at regulating carbon, fat, protein and water metabolism.
Literature 1. Glinchuk Ya.I., Deev L.A. Ophthalmosurgery. 1990. 2. 42–47. 2. Kalinin A.P., Nurmanbetov D.N., Mozherenkov V.P. Changes in the organ of vision in endocrine diseases: Educational and methodological manual. Frunze, 1988. 3. Kalinin A.P., Mozherenkov V.P., Prokofieva G.L. Ophthalmoendocrinology. – M.: Medicine, 1998. – 160 p. 4. Mozherenkov V.P., Kalinin A.P. Ophthalmological Journal. 1991, I. 54–58. 5. Mozherenkov V.P., Kalinin A.P., Prokofieva G.L. Changes in the organ of vision due to endocrine disorders: Textbook. – M., 1993. 6. Nesterov A.P. Diabetic lesions of the organ of vision // Current problems of endocrinology: Proc. report III All-Russian Congress of Endocrinologists. – M., 1996. – P. 78–79.
How to avoid diabetes if your sugar is a little high?
If your blood sugar is a little high, exercise
The human body, like all living things in the world, is subject to change. Each person has their own sugar threshold. How to avoid diabetes if your sugar is a little high? There is no need to worry if you have such a problem, but you need to act correctly.
- As mentioned above, the cause of increased sugar can be various conditions of the body or life situations.
- This may be due to the improper functioning of some organs in the body. You need to undergo an examination, which the doctor will additionally prescribe for you.
- We can also talk about chronic or one-time stress. Try to calm down or take a sedative such as Valerian or Corvalol.
- Eating too many sugar-containing foods before testing can also have an effect. If, for example, you ate cake the day before the sample was taken, this may distort the test result. In this case, repeat the analysis in a couple of days.
But it is worth noting that sometimes when we are talking about an increase in sugar, we are talking about something else:
- Blood sugar levels in men and women depend on age.
- In older people, sugar levels also increase. On average, in people 50–60 years old it should be up to 6 mmol/l.
- In women, sugar levels depend on hormonal levels. For example, pregnant women during the perinatal period showed that their blood sugars would be higher than when they were not pregnant.
All doctors say that you should eat normally before the test, but it is still advisable to eat less sugar before the day of blood donation. This will show a more complete and correct picture.
More important tips:
- Play sports
- Eat right
- Get rid of excess weight
- Eliminate sugar-containing foods from your diet
- Avoid fatty and fried foods
- Avoid foods with a high glycemic index.
High glycemic index foods
You can also use recipes from traditional medicine to stabilize blood sugar:
- Drink decoctions and infusions from blueberry, clover, and nettle leaves. Pour one tablespoon of the mixture into a glass of water, strain after 20 minutes and drink 1/3 glass 3 times a day.
- You can use bean pods, calamus root, corn silk, or regular chamomile flowers. Decoctions from these plants will relieve inflammation and improve the functioning of the liver and pancreas.
- Chamomile tea improves the general condition of the body and usually does not harm a person in any way. But be careful: if you are allergic to chamomile, you should not drink this tea.
Of course, at the first discomfort you should consult a doctor. But you can try to improve blood sugar and the state of the digestive system as a whole, and eliminate mild infections at the initial stage on your own. Traditional medicine recipes are a great help. However, if the condition worsens, do not put off visiting a doctor, otherwise all this can lead to complications that are difficult to treat.
Diabetic macular edema
This complication of diabetic retinopathy is called one of the most significant causes of decreased central vision. The macula is important for clear, straight-line vision, which is used for reading and recognizing faces. Most often, swelling occurs in patients with type 2 diabetes mellitus and can appear at any stage of diabetic retinopathy, but most likely already at a fairly advanced stage.
The formation of macular edema is promoted by: microthrombosis of capillaries and increased permeability of retinal vessels
Based on the area of the lesion, edema is usually divided into focal and diffuse. Focal edema outlines a local zone of fluid leakage from microaneurysms and vessels, and diffuse edema implies hyperpermeability of the entire capillary network. Due to edema, thickening of the retina occurs, and in some places diffuse damage causes the formation of cysts in the retina. Visual acuity decreases, and degeneration of the retinal pigment epithelium may develop.
First signs and symptoms
Deformation and dystrophy of the eye organs in diabetes mellitus occurs very slowly, therefore, at the initial stages of the development of these processes, the patient himself does not notice significant changes in visual perception. For several years, vision may be good, pain and other signs of any disorders may also be completely absent.
And when pathological processes have already reached a certain phase of their development, the patient may experience the following symptoms:
- a veil before the eyes;
- dark “spots” or “goosebumps” before the eyes;
- reading difficulties that were not previously observed.
These are the first symptoms that indicate that the pathology has already begun to actively progress and the time has come to treat it. But often many diabetics do not attach importance to these changes in visual perception and do not take any measures.
However, it gets worse and worse. Vision gradually decreases, headaches appear from overstrain of the eye muscles, pain in the eyes and a feeling of dryness occur. And it is at this stage that patients most often go to the doctor and undergo an examination, which allows them to identify the development of retinopathy.
Diagnostic measures that are carried out to identify pathological processes in the eyes may include:
- checking visual acuity and identifying its boundaries;
- ophthalmological examination of the fundus using special instruments;
- measurement of intraocular pressure;
- Ultrasound examination of the fundus.
It should be noted that most often vision problems occur in those people who have had diabetes for many years (20 years or more). But in medical practice there have been numerous cases when the diagnosis of diabetes mellitus occurs against the background of poor vision.
First signs of vision loss
Vision deterioration in diabetes occurs gradually and lasts for years. That is why the addition of one symptom after another may not bother a diabetic who is simply getting used to his current condition. However, the clinical picture is assessed by ophthalmologists as more than pronounced:
- violation of the contrast of visual functions, for example, if vision is better in the evening than during the day;
- spots or rainbow circles before the eyes;
- changing the boundaries of the visual field for no reason;
- decrease in visual function by one diopter per year (this is the so-called progressive “minus”);
- dryness, insufficient tear production.
Acute and chronic complications of diabetes mellitus type 1 and 2, their prevention
At later stages or in case of rapid progression of the condition, a diabetic may experience sharp pain in the eye area, which can lead to nausea or even vomiting. A burning sensation, sand in the eyes, the sensation of a foreign object - all this indicates that vision is deteriorating before the eyes, and therefore it is necessary to begin treatment as soon as possible.
Cataract
The possibility of lens clouding increases with the duration of diabetes. A cataract goes through several stages of “maturation”, during which the lens thickens and increases in size: initial, immature, mature and overripe (mammary).
The causes of cataracts in diabetes mellitus are increased sugar levels in the blood and chambers of the eye, impaired blood supply and nutrition to the lens, damage to nerve fibers due to endocrine disorders
True diabetic cataract is more typical for the younger age group with juvenile uncompensated diabetes. It develops rapidly, over a few days, and affects both eyes at once. If you identify this process in time, then by normalizing carbohydrate metabolism, you can reverse the process. If this is not done, then further maturation of the cataract occurs and the lens becomes uniformly clouded. Myopia develops. Dystrophic processes and microcirculation disorders occur in the iris.
Causes of diabetes
The lens is located inside the eyeball and is a vitreous body that transmits light rays. They, falling on the retina, show the images they saw.
In diabetics, excess sugar enters the visual organs. Glucose, after processing, becomes fructose, resulting in the production of sorbitol. As a result, osmotic pressure increases, metabolic processes and microcirculation are disrupted. All these indicators contribute to the lens becoming cloudy.
Diabetic cataracts are caused by the following reasons:
- impaired blood circulation in the eyeballs,
- insufficient insulin levels,
- eyelashes swell,
- acidosis,
- endocrine disorders,
- increased sugar.
The disease progresses much more rapidly in insulin-dependent patients.
Cataracts can occur when excess sugar and acetone in the lens increase the light sensitivity of the protein. This causes the natural protein structure to change and the lens to become cloudy.
Effects of diabetes on the eyes
The small and fragile blood vessels present in the retina of the eye can also be damaged if blood sugar levels remain persistently high for a long period of time. The small capillaries in the retina weaken and swell to the point that they collapse.
Despite the appearance of new blood vessels, during hyperglycemia most of them are damaged and their weakened walls allow blood to pass through.
This can lead to diabetic retinopathy, one of the many complications associated with uncontrolled diabetes. In addition, uncontrolled diabetes can cause swelling of the lens, which can impair vision.
Hyperglycemia can also cause blurred vision and increase the risk of developing cataracts, glaucoma, and even blindness.
The effect of diabetes on the heart and cardiovascular system
In the long term, diabetes mellitus significantly increases the risk of developing coronary heart disease (CHD), myocardial infarction, and other cardiovascular diseases. Diabetes can lead to the deposition of fatty clots (cholesterol plaques) on the inner walls of blood vessels. With atherosclerosis, blood vessels become clogged with blood clots, making them narrow and fragile. This impairs blood circulation and causes the development of hypertension, atherosclerosis, coronary heart disease, heart attacks, cerebral vascular diseases and strokes.
About the impact of diabetes on the heart, read the articles: Diabetes and stroke and Foods high in cholesterol - tips for diabetics on replacing them.
Effects of high sugars on the nervous system
Neuropathy, or nerve damage, is one of the most common complications associated with diabetes. This disease is known as diabetic neuropathy. Having excess sugar in the blood can damage the small blood vessels that supply blood to the nerves.
Nerve endings present in the extremities of the body (arms and legs) are particularly susceptible to the negative effects of hyperglycemia.
Over time, many diabetics begin to experience numbness, throbbing, and tingling in their hands and feet, as well as decreased sensation.
This is especially dangerous for the legs, because... if a diabetic can no longer feel his toes and feet and they can easily become damaged and also become deformed. With the development of diabetic neuropathy, a decrease in sexual function is also observed.
Impact of diabetes on skin, bones and feet
People with diabetes are much more likely to suffer from skin conditions such as fungal and bacterial skin infections, along with bone and joint problems such as osteoporosis.
As mentioned, high blood sugar levels cause damage to nerves and blood vessels, especially those present in the extremities of the body. This ultimately leads to various foot problems, the most serious of which is diabetic foot syndrome.
Read more about the negative effects of diabetes on the legs and feet: Diabetic foot as a dangerous complication of diabetes - symptoms, treatment, photos
Diabetes mellitus and ketoacidosis
In addition to the above-mentioned chronic complications, poorly managed or uncontrolled diabetes can cause diabetic ketoacidosis.
Diabetic ketoacidosis is a condition in which ketone bodies begin to accumulate in the body. When cells are unable to utilize glucose from the blood, they begin to use fat for energy. The breakdown of fats generates ketones as by-products. The accumulation of large amounts of ketones increases the acidity of the blood and tissues. This leads to serious complications if a patient with developed ketoacidosis does not receive appropriate treatment. In case of ketoacidosis, the patient should be hospitalized immediately, because this complication is life-threatening and is treated mainly with droppers, and also because an urgent adjustment of insulin doses and nutrition is required. At the initial stage of development of ketoacidosis, it is recommended to bring blood sugar back to normal and consume large amounts of mineral water to reduce blood acidity.
Conclusion
In order to delay the onset of chronic complications of diabetes and prevent its short-term negative manifestations, it is necessary to keep blood sugar levels normal. This is the most important recommendation for patients with diabetes.
Effective management of diabetes is only possible when medications are combined with proper nutrition, weight management and regular physical activity.
How to avoid losing vision with diabetes
If problems with glucose absorption are diagnosed, then when visiting a patient with diabetes, the doctor gives recommendations on how to avoid complications, including those affecting the eyes:
- You need to constantly check your blood sugar levels. With a glucometer on hand, measurements can be taken daily at home;
- Follow the principles of nutrition to exclude the possibility of increased glucose;
- Take tablets or injections depending on the type of diabetes;
- Visit an ophthalmologist annually to promptly detect changes in the eye vessels and carry out complex therapy;
- Do not neglect the recommendations of an endocrinologist, ophthalmologist and other specialists in order to avoid serious consequences in the form of irreversible loss of vision.
If all conditions are met, then the effect of diabetes on vision will not be dangerous and the person will not lose the ability to see the world around him in all its bright colors.
Glaucoma
An increase in intraocular pressure occurs due to a combination of several factors, but in the case of diabetes mellitus, the leading positions are occupied by the following points:
- poor circulation due to diabetic retinopathy;
- hypoxia and ischemia of eye tissue due to swelling and multiple hemorrhages;
- disruption of the outflow of aqueous humor. Most often, at the proliferative stage of retinopathy, new vessels grow into the iris of the eye and affect the normal outflow of moisture through the anterior chamber.
The main pathological changes occur at the exit site of the optic nerve. Since intraocular pressure is increased, compression of the nerve endings occurs in this area, and the disc even bends slightly. With a prolonged course of the disease, atrophy of the optic nerve occurs and the patient loses vision. This happens gradually, first the boundaries of the blind spot expand, then the area of arcuate vision loss increases. Peripheral vision from the side of the nose gradually disappears, then it may disappear completely. This means complete atrophy of the optic nerve.
Characteristic narrowing of the visual field in glaucoma
Although some researchers believe that some of the nerve fibers are in the “sleep” stage and with intensive treatment, vision can be restored.
Preventing vision loss in diabetes
The main thing that is necessary to minimize the rate of vision deterioration:
- Monitoring blood glucose levels and blood pressure. Regular clinical and laboratory examination by an endocrinologist, mandatory compliance with all points of diabetes therapy. They include drug therapy, diet, maintaining a proper lifestyle
- Regular examination by an ophthalmologist. It needs to be done 2 times a year and when signs of visual impairment appear. This is important for early diagnosis of pathological changes and initiation of timely treatment.
Compliance with these points will help reduce the rate of loss of vision and partially restore already lost visual properties.
Treatment
Therapeutic therapy begins with the fact that the main disease – diabetes mellitus – is first cured. To achieve this goal, the following tasks are solved:
- glucose levels are normalized,
- the optimal dose of insulin and medications that reduce sugar is selected,
- metabolism is adjusted,
- a healthy lifestyle without bad habits is organized.
Diabetics should visit an ophthalmologist at least once every 6 months.
To reduce high sugar levels, eye drops “Quinax” and “Catachrome” are used. For preventive purposes, they are used for a month, after which the same break is taken and the course is repeated. Sometimes therapy lasts a lifetime to prevent surgery. Eye drops are not able to stop the disease, they only slow down its progression.
Diabetic cataracts are completely eliminated through surgery; there are no other effective methods. It is recommended to remove the lens at earlier stages, without waiting for the disease to become advanced.
It develops quite quickly, so the patient may suddenly begin to see worse. The use of contact lenses and glasses in this situation does not correct vision.
If it is necessary to perform cataract surgery for diabetes mellitus at the onset of the disease, phacoemulsification is used. It should be borne in mind that visual acuity should not decrease by more than 50%. The advantage of this type of intervention is that there is no need to apply stitches; therefore, astigmatism does not develop after it.
Eye surgery consists of the following: a micro-incision is made with a laser or ultrasound, through which the deformed lens is removed, leaving the capsular bag. An intraocular lens is placed instead of the natural lens. The procedure is done using local anesthesia.
Patients note that improvement appears immediately, despite this, the recovery period lasts some time. If the lesion affects both eyes, first remove the film from one eye, then after about 3 months from the other.
There are some reasons prohibiting the operation:
- advanced stages of retinal pathologies,
- formation of a vascular network on the iris,
- blindness,
- inflammation of the visual organ.
Before surgery, it is necessary to confirm that blood glucose levels have returned to normal and that the patient does not have chronic diseases that could interfere with postoperative rehabilitation.
The operation is performed on an outpatient basis, the tissues and blood vessels of the eye are not injured, and vision is restored on the second day. After the procedure, it is recommended to use hormonal and non-steroidal drops.
Diagnostics
We also recommend reading: Retinal vascular changes
Depending on the severity of diabetes, it is necessary to undergo an ophthalmological examination every six months to a year. The main methods for studying the condition of the eye are ophthalmoscopy (using an ophthalmoscope device, the condition of the optic nerve, retina, and blood vessels is visually assessed) and fluorescein angiography of the fundus (FAGD).
FAGD involves intravenous administration of a contrast agent. Then the doctor examines the condition of the eye vessels in the light of a special lamp. If there are ruptures and microbleeds, a fluorescent substance will help to notice them.
A specific research method - perimetry - is used to determine visual fields, this helps to identify damage due to glaucoma or macular edema.
Retinal tomography and ultrasound biomicroscopy are used to assess the condition of the optic nerve and retinal thickness.
Fundus examination
The stages described above occur sequentially one after another. Regular fundus examinations are needed precisely in order to understand the condition of your retina and not miss the moment when something else can be done to prevent or slow down the progression of complications.
The retina and its vessels can be seen by examining the fundus of the eye. This examination is performed by an ophthalmologist. In order to conduct it efficiently, you must first drip drops into your eyes that dilate the pupil - this will allow you to get a greater overview and see all the changes in the fundus.
The fundus is the structures visible when examining the eye, which include the retina with its vessels, the optic disc, and the choroid.
Often in clinics, ophthalmologists simply assess visual acuity and measure intraocular pressure. However, remember, if you have diabetes, it is in your best interest to know the condition of your retina. Do not consider it difficult to remind the ophthalmologist about your disease and that it is time to conduct a fundus examination with a dilated pupil. After the examination, depending on the condition of the retina, the doctor will determine the frequency with which you will need to undergo regular examinations. This may be once a year, or maybe at least 4 times a year - it all depends on each specific case.
In some cases, fluorescein retinal angiography .
This study is carried out in specialized ophthalmology clinics. Fluorescein angiography makes it possible to identify changes in blood vessels that are invisible during normal examination, the degree of their occlusion, areas of insufficient blood supply, helps to distinguish microaneurysms from hemorrhages, determine the permeability of the vascular wall and the exact location of newly formed vessels.
Methods of therapy
Treatment of the visual organs for hyperglycemia involves the primary normalization of carbohydrate and protein metabolism. The endocrinologist will help create a competent diet for the patient, select drugs that stabilize sugar, and if they are not effective, prescribe insulin injections. Additionally, it is necessary to take medications to reduce blood cholesterol and blood pressure, as well as vascular strengtheners and vitamins. If we are talking about inflammatory processes (barley, blepharitis, conjunctivitis, etc.), then first of all the source of infection is sanitized. The ophthalmologist selects local ointments and drops to reduce symptoms, and general anti-inflammatory drugs for oral administration. But it is necessary to take into account that such drugs can again increase the concentration of sugar in the blood. Treatment of keratitis is often accompanied by complications, such as trophic ulcers, clouding of the cornea and others.
Neovascular glaucoma with high sugar is difficult to treat. First of all, the doctor selects drugs to reduce intraocular pressure, but the sharp deterioration of vision in diabetes can only be stopped through surgery. The surgeon artificially creates drainage paths for intraocular fluid to compensate for the pressure. And the destroyed vessels are coagulated using a special laser.
Cataracts also require surgical treatment. The surgeon performs phacoemulsification of the clouded lens and implants an artificial lens.
Retinopathy in diabetics is treated with periodic laser coagulation of the retinal capillaries. The procedure allows you to limit the area of edema and prevent the destruction of new vessels.
Stages of development of retinopathy
In total, there are 4 stages of development of retinopathy:
- background retinopathy;
- maculopathy;
- proliferative retinopathy;
- cataract.
Stages of development of diabetic retinopathy
Background retinopathy
This condition is characterized by damage to the small capillaries of the fundus and changes in the limbus. Its peculiarity is that it does not manifest itself in any way. And in order to prevent the transition of background retinopathy to other forms of the disease, it is necessary to constantly monitor blood sugar levels.
Maculopathy
At this stage of the development of the disease, the patient is diagnosed with lesions of the macula, which plays a large role in the process of a person’s perception of the surrounding world through images. It is at this stage of retinopathy that, as a rule, there is a sharp decrease in vision in a diabetic.
Proliferative retinopathy
This condition is characterized by insufficient oxygen supply to the vessels supplying the eye organs, as a result of which new vessels begin to form on the back surface of the fundus of the eye, leading to its deformation.
How to protect your vision
Vision loss from diabetes is sometimes irreversible. But early detection of the disease and comprehensive treatment can reduce the risk of blindness by 95%.
Since in the early stages eye diseases do not yet have pronounced symptoms, their examination in patients with diabetes mellitus should be carried out preventively regularly every 2-4 months. The usual tests that people with diabetes undergo are general and biochemical blood tests, glycosylated hemoglobin, C-peptide and urinalysis.
Controlling diabetes through diet, carbohydrate regulation, and medications significantly delays the onset and reduces symptoms of retinopathy
The main goal of treatment for the underlying disease is to maintain blood sugar levels as close to normal as possible, control high blood pressure and lower cholesterol.
Formed diabetic eye pathologies can be treated with several methods, which are used individually and in combination.
Vascular growth factor blocking drugs
In response to damage, retinal pigment epithelial cells secrete vascular growth factor to promote the formation of an additional network of blood vessels. Drugs that inhibit this factor are injected into the vitreous body. They suppress pathological revascularization, reducing the likelihood of retinal bleeding and swelling. Today this group of medications includes:
- Pegaptanib (Macugen, Eyetech Pharmaceuticals⁄Pfizer).
- Ranibizumab (Lucentis, Genentech⁄ Roche).
- Bevacizumab (Avastin, Genentech⁄ Roche).
Drugs that block vascular growth factor - a new word in the treatment of diabetic retinopathy
Most people require monthly injections of these medications for the first six months of treatment. After this, injections are needed less frequently: usually three or four during the second half of treatment, about four during the second year of treatment, two in the third year, one in the fourth year, and none in the fifth year. This scheme has a beneficial effect on vision.
Corticosteroids
Corticosteroids injected or implanted into the eye may be used alone or in combination with other medications or laser surgery. In world practice, the Ozurdex implant (dexamethasone) is used for short-term use, and the ILUVIEN® implant (fluocinolone acetonide) is used for a longer period. Both are biodegradable and release a stable dose of corticosteroids to suppress retinopathy. The use of corticosteroids in the eye increases the risk of developing cataracts and glaucoma, so intraocular pressure should be monitored during treatment with these drugs.
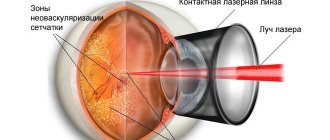
Focal/mesh macular laser surgery
This treatment method involves laser photocoagulation of damaged blood vessels, after which they stop bleeding. Such cauterizations also reduce retinal swelling. The surgery is usually a one-time procedure, but some patients may need a couple of sessions. The doctor can do 1000 to 2000 cauterizations, pressing down the central area. This allows you to preserve central vision.
Laser coagulation is recognized worldwide as the gold standard for surgical treatment of diabetic retinopathy.
A laser is sometimes used before injections of drugs that block vascular growth factor. And sometimes only if macular edema does not decrease after treatment with anti-VEGF drugs for 6 months.
Another direction of laser surgery is “adhesion” for retinal detachment. It is used both as a therapeutic measure and as a preventive measure.
Laser correction is also used for glaucoma. By means of laser iridotomy and trabeculoplasty, the outflow of intraocular fluid through natural pathways is restored.
Vitrectomy
In case of significant hemorrhages in the vitreous body, its removal is required. This procedure is called vitrectomy. In the process, through special holes using a vitrector device, a saline solution is first supplied into the eye chamber to maintain constant pressure, then the damaged vitreous body is removed and replaced with a new one (made of liquid silicone, perfluorocarbon). This operation also allows you to remove scars and seals. If the procedure is required for both eyes, the second is usually treated after the first has fully recovered.
In case of detachment, you can resort to this operation to provide additional pressure on the retina.
Extrascleral filling
A surgical intervention that aims to ensure a tight fit of the retina to the vascular layer. It is carried out in the area of fresh detachment. The filling is prepared from a special spongy silicone according to the size of the peeling area, placed in the sclera and fixed there with sutures.
Retinal detachment requires immediate surgery
A variety of methods for treating eye diseases in diabetes mellitus today makes it possible to preserve or improve the vision of patients. The most important task of the patient himself is to carefully consider any changes in vision and immediately undergo an examination.