About 70% of urethral injuries occur as a result of road traffic accidents, 25% as a result of a fall from a height, and 5% as a result of other factors, including iatrogenic ones. There are closed (subcutaneous) and open injuries, as well as isolated and combined injuries of the urethra. 96% of victims have closed injuries and only 4% have open ones (16)
Therapeutic tactics in the acute period of urethral trauma are one of the cornerstones of modern emergency urology. It is widely believed that open urethroplasty in the next 24 hours after urethral rupture is not indicated due to poor tissue visualization and differentiation of anatomical structures. Due to the presence of hematoma, edema and urinary infiltration, it is impossible to accurately determine the degree of damage to the urethra, and precise comparison of anastomotic surfaces is difficult. According to a number of authoritative sources, with early urethroplasty, the incidence of postoperative strictures ranges from 45 to 83.3%, erectile dysfunction - up to 20% (17). The risk of stress urinary incontinence reaches 18% (15). Webster GD and co-authors believe that the method has the right to exist in exceptional observations, when the so-called high location of the prostate, concomitant damage to the rectum and bladder neck, as well as ongoing bleeding are detected (6). However, RP Shrinivas and D Dubey, comparing the results of urgent and delayed urethroplasty for injuries of the posterior urethra, come to the conclusion that the postoperative complications described above are not due to the timing of the intervention, but to the severity of the injury itself (18).
The method of choice for urethral ruptures is currently cystostomy, and, if possible, urethral catheterization and drainage of hematomas. The reconstructive stage is performed approximately after 3-6 months, depending on the severity of the injury and the condition of the surrounding tissues (1,3,4,5,7,8,9).
10-14 days after drainage of the bladder using a cystostomy installed immediately after the injury, it is possible to perform delayed primary urethroplasty, since during this time the hematoma resolves. Urethroplasty is performed by endoscopic, abdominal or perineal access. Primary urethroplasty provides an 80% favorable outcome without the formation of strictures. This method is also considered the best option for the treatment of urethral injuries in women, which makes it possible to maintain normal urethral length and urinary continence (2,10,11,12,13,14).
Results and discussion
Over the past years, the team of the urology clinic at the Research Institute of Uronephrology and Reproductive Health of the Ministry of Health and Social Development of the Russian Federation has been actively working to improve the results of treatment of patients with various types of disorders of the integrity of the urethra.
We present a clinical observation in which, due to circumstances, the features of surgical tactics do not fit into modern canonical ideas about the treatment of patients with injuries to the urethra.
Patient G., 65 years old, August 12, 2013 - fell onto a metal beam from his own height. Due to the inability to urinate independently, puncture cystostomy was performed on the same day. In the postoperative period, pronounced swelling of the scrotum was noted; ultrasound and MSCT (Fig. 1) revealed a hematoma of the perineal tissue spreading to the right half of the scrotum.
Figure 1. Computer tomogram. CT image of a scrotal hematoma with a total volume of 300 ml.
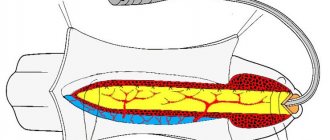
X-ray examination revealed a rupture of the bulbous urethra (Fig. 2). On August 18, 2013, the right half of the scrotum was revised and the hematoma was removed. During the operation, the hematoma with membranes was mobilized, opened, and 300 ml of blood clots were evacuated. Imbibition of the beginning of the bulbous section of the corpus spongiosum of the urethra was detected; no signs of ongoing bleeding were established.
However, on August 20 and 21, repeated bleeding into the bladder cavity was observed.
On August 22, due to ongoing bleeding, the patient underwent cystotomy.
Fig. 2. Antegrade cystogram and retrograde ureterogram: it was established that the tightness of the bladder was not broken. Rupture of the bulbous part of the urethra, leakage of contrast agent into the paraurethral tissue.
On August 25, cystotomy and revision of the bladder revealed ongoing arterial bleeding from the internal opening of the urethra. Attempts to ante- and retrogradely pass the catheter through the urethra without effect.
Considering the life-threatening bleeding, a decision was made to inspect the urethra.
Among the features of the surgical intervention, an incision was made in the perineum from the lithotomy position with a transition to the root of the scrotum 8 cm long. The bulbous part of the urethra was mobilized. It was established: traumatic damage to the corpus spongiosum of the urethra over 5 cm, crushing and “old” imbibition of the bulbospongiosus muscles with blood. Necrotic and crushed tissues were excised. It was established: damage to the urethra at the level of the proximal portion of the bulbous section. Mobilization of the urethra over 8 cm, crossing it directly in the area of damage. Search for the source of bleeding - established: bleeding from the bulbous arteries - stopped by ligation.
Resection of necrotic tissue of the urethra. Upon examination, it was established: urethral diastasis is about 3 cm. Taking into account the possibility of repeated bleeding, the presence of mobilized areas of the urethra, sanitized from necrotic and imbibed with blood, as well as extremely negative prospects for subsequent reconstructive operations (under such circumstances, the probability of extended obliteration and lifelong cystostomy is extremely high) a decision was made to perform anastomotic urethroplasty.
The intercrural space is cut and urethral diastasis is compensated. A urethro-urethroanastomosis was formed without signs of tension, using 8 Vicryl 3-0 anastomotic sutures. Drainage of the urethra with catheter No. 16, of the bladder with a cystostomy. Drainage of the paraurethral zone with silicone drainage, active aspiration.
The postoperative period was uneventful. The drainage was removed on the 3rd day. The wound healed by primary intention.
In Fig. Figure 5 shows the results of retrograde urethrography 2 weeks after surgery and removal of the urethral catheter.
Fig 5. Retrograde urethrogram. In the areas of anastomosis, a slight unevenness of the contours of the urethra is determined, there is no narrowing.
The urethral catheter was removed.
The cystostomy has been removed. With uroflowmetry, the maximum urine flow is 16 ml/s, the average is 9.2 ml/s with 180 ml of urine.
A repeat urethrogram after three months showed no significant differences (Figure 6).
Figure 6. Urethrogram 3 months after surgery
Urethral injury
Conservative management is allowed in the presence of non-penetrating bruises, sprains and the provision of specialized care no later than 6-12 hours after receiving a traumatic injury. The optimal solution in such cases is to provide rest, apply cold, prescribe NSAIDs that have anti-inflammatory and analgesic effects, hemostatic drugs, sedatives and tranquilizers. To prevent possible infectious complications of injury, preventive antibiotic therapy is carried out. If urination is impaired, a rubber catheter is installed for up to 7 days. In other cases, surgical treatment is recommended.
When choosing an operation, the severity of the patient’s condition and the characteristics of the traumatic injury (location, severity, type, combination with other injuries) are taken into account. The main objectives of surgical intervention are to ensure unimpeded urine flow, create conditions for the healing of damaged tissue, or reconstructive restoration of the urethra. The main types of operations for traumatic destruction of the urethra are:
- Suprapubic epicystostomy
. In case of partial ruptures, urine diversion through a cystostomy can reduce the load on the walls of the urethra; in case of complete ruptures, it can eliminate acute urinary retention. Depending on the degree of damage, epicystostomy is supplemented with catheterization of the bladder or reconstructive urethroplasty, corresponding to the type of damage. - Primary urethrourethroanastomosis
. Comparison of the rupture is possible if there is a slight divergence of its ends, the absence of massive urohematomas, and the patient’s condition is satisfactory. The advantage of a primary urethral suture is the low likelihood of erectile dysfunction. Intervention is often performed for injuries to the spongy part of the organ. - Delayed catheter-based urethroplasty
. The urethra is catheterized for 2-3 weeks with a tube made of biologically inert material, which is installed through a high section of the bladder. The wall defect is sutured after the patient’s condition has stabilized. Delayed interventions are recommended for posterior injuries.
Patients with open injuries undergo primary surgical treatment of the wound. In the presence of urinary leaks, urohematomas ensure their opening and drainage. The complicated course of the traumatic process often requires late reconstructive plastic surgery to eliminate strictures, fistulas and other long-term consequences.
conclusions
Anastomotic repair in a patient with extensive damage to the urethra was performed on the 10th day from the moment of injury. Satisfactory results of the operation can, to one degree or another, be due to adequate surgical sanitation of the urethral bed with complete removal of softened tissue, as well as adherence to the principles of microsurgical technique at the reconstructive stage. However, despite the results obtained, the operation was of the nature of desperation and such tactics in no way pretend to change the established canons in the treatment of patients with urethral injuries and can only be applied in exceptional, forced situations by surgeons who know the principles of urethral surgery.
Diagnosis of the disease
The diagnosis is made based on the methods of urethrography and X-ray with contrast, monitoring of patients and drawing up a clinical picture of the course of the disease. In case of urethral rupture, catheterization is a contraindication, as it can cause complications. When the posterior sections - prostatic and membranous - are ruptured, urination is observed only according to the urge. If the bladder ruptures, it occurs spontaneously. This fact makes it possible to diagnose rupture of urethral tissue. If it is not possible to determine the location of the rupture, then they resort to urethrography and x-rays. If X-rays are used, the location is localized according to the leaked radiopaque fluid from the urethral area.
Examination methods
The urologist determines the parameters of the state of the urinary system; during a consultation, examining the damaged area and taking into account the patient’s complaints, he uses the following examination methods for an expanded diagnosis of pathology:
- acoustic scanning, which displays the structural characteristics of the organs being studied, their sizes, pathological deviations;
- urethrography provides full visibility of the structural parts of the organ upon administration of an indicator substance, followed by an x-ray;
- Computer tomography makes it possible to obtain a three-dimensional view of the organ under study, with the ability to examine adjacent tissues and systems, identifying bone damage and hemorrhages;
- surface endoscopy is used for minor urethral trauma
, which does not violate the integrity of the structure, allowing you to characterize the internal state using optical magnification of visual inspection;
- laboratory testing of blood and urine characterizes the general condition of the body, the possible presence of inflammation of the urinary tract, and the presence of internal bleeding.
Therapeutic measures are determined by the urologist
based on the results of the diagnostics, which include the use of conservative methods for relieving the condition in case of minor damage or surgical intervention that restores the integrity of the structure of the urethral canal.
Causes and mechanisms of occurrence
The conditions for the origin of urethral ruptures are divided into individual areas:
1. In the stem part;
2. In the perineal-bulbous part;
3. In the membranous part;
4. In the prostate part.
Stem ruptures
They can occur in a healthy or diseased urethra, with a relaxed shaft or in a state of erection. If the unchanged walls of the urethra have all their elasticity and the shaft sags in an unstressed state, then there is little chance of a rupture forming. In a state of erection, the penis is more often the object of damage that involves the urethra from the very beginning or spreads to it in a secondary way: this includes bites, twisting, blows, and pinching. If the urethra is inflamed and its walls have become brittle as a result, then the chances of rupture increase, and they reach their maximum when the shaft is in a state of erection. Rough straightening of the shaft, even less force, such as a rapid erection that does not allow the curved urethra to follow the expansion of the cavernous bodies, can then easily cause a violation of the integrity of the urethra.
Ruptures of the perineal-bulbous part
This is a classic urethral injury. All its causes come down to damaging bodies that act on the perineum, which is at rest, or which are encountered by the perineum, which is in motion. In the first category of cases, we are talking about a blow delivered from behind with a stick, a hammer, a human foot or a horse's hoof. In cases of the second category, the injury occurs due to a fall with the perineal area on a tight rope, on a log, on a ladder, on a board, on a bicycle frame.
As for the mechanism of these ruptures, they can be divided into: cases when the damaging body acts on the perineum, which is at rest; cases when the perineum, while in motion, encounters a damaging body.
In cases of the first kind (a blow from a stick, a human foot, or a horse's hoof, applied from behind), the bulb may be, so to speak, caught and torn off at the level of the membranous part, or it may burst due to the blood contained in its cavities being equally incompressible. with any liquid, breaks their partitions.
In cases of the second type (falling astride a rope, onto a log), the urethra is ruptured due to pinching between the damaging body and some support point lying outside it.
Membranous part ruptures
Rupture of the membranous part in most cases is the result of a fracture of the pelvis and occurs due to tugging of the middle aponeurosis by displaced fragments, or due to perforation of the urethra by a bone fragment.
Prostate tears
Regardless of major injuries involving the pelvic skeleton and accompanied by such severe disorders that damage to the urethra goes unnoticed, ruptures of the prostatic urethra are extremely rare.
General symptoms
Signs of injury may differ slightly in patients of different genders. However, it is possible to identify common manifestations of urethral rupture in men and women:
- difficulty urinating;
- hematoma in the perineum and genital area;
- soreness in the urethral area;
- reddish impurity in the morning urine;
- discharge of blood from the urethra between urinations.
Hematuria (blood in the urine) is not necessarily a sign of organ damage. With a partial rupture, bleeding may not occur if there is no destruction of the vessels. But even in the absence of bleeding, injuries to the urethra are always accompanied by severe pain in the perineum.
With a complete rupture of the urethra, additional symptoms appear:
- Disappearance of urination. If parts of the urethra are completely separated from each other, then emptying the bladder naturally becomes impossible.
- Pain and heaviness in the lower abdomen. These symptoms occur due to an overfilled bladder.
Features of injury in women
When women are injured, a partial rupture of the urethra most often occurs. Complete separation of parts of the urethra from each other is extremely rare.
As already mentioned, women receive similar injuries during pelvic fractures or difficult childbirth. Often, in patients, not only the urethra is damaged, but also a nearby organ - the vagina. A rupture of the anterior vaginal wall occurs. A sign of such damage is the release of urine from the genital tract. This is accompanied by acute pain in the perineum, which intensifies when in a sitting position.