Live broadcasts on Instagram every Sunday at 12:00
Subscribe so you don't miss out! Subscribe
- home
- Urology
- Nephroptosis (prolapse of the kidney)
Patent. Method of laparoscopic nephropexy
Nephroptosis (prolapse of the kidney) is excessive mobility and rotation of the kidney that occurs in an upright position of the body. Normally, during breathing and when the body moves, both kidneys move within the acceptable physiological norm, which should not exceed the height of the lumbar vertebral body (2–4 cm). Normally, the right kidney is located slightly lower than the left kidney. Nephroptosis is considered to be a displacement of the kidney in a vertical position of the body downward by more than 2 cm, and with a deep breath - by more than 3-5 cm; in addition, nephroptosis also refers to a condition in which the kidney rotates around the vascular pedicle.
The following degrees of nephroptosis are distinguished:
- I degree of nephroptosis - prolapse of the lower pole of the kidney more than 1.5 lumbar vertebrae
- II degree of nephroptosis - prolapse of the lower pole of the kidney of more than 2 vertebrae
- III degree of nephroptosis - prolapse of the lower pole of the kidney of more than 3 vertebrae
When a kidney prolapses, it can either remain stably low compared to the physiological norm, or return to its place when the body position changes - the so-called “migrating kidney”.
To determine the degree of nephroptosis and the severity of kidney dysfunction, as well as to choose the correct surgical treatment tactics, you must send me a complete description of standing and lying ultrasound of the kidneys, standing and lying ultrasound of the kidney vessels, intravenous urography and radioisotope scintigraphy data [email protected] kidneys, indicate age and main complaints. Then I will be able to give a more accurate answer to your situation.
Prevalence of the disease.
Nephroptosis is a fairly common disease (from 0.07 to 10.6%), occurring in people in the prime of life (20–40 years) (Baran E.E., 1990; Lopatkin N.A., 1998; Lopatkin N. A. et al., 1985). Right-sided nephroptosis is most common. In women, kidney prolapse occurs almost 15 times more often (1.5% of people over 18 years of age) than in men (0.1%). This fact is explained by the structural features of the female body - a wider pelvis, reduced tone of the abdominal wall, greater elasticity of the ligaments. Bilateral nephroptosis is observed relatively rarely.
Reasons for the development of nephroptosis.
Normally, the kidney is fixed in its typical place thanks to the ligaments, surrounding fascia and fatty tissue. The most common factors that can lead to the development of nephroptosis (prolapse of the kidney) include sudden weight loss, decreased muscle tone of the abdominal wall, trauma to the lumbar region, constant carrying of heavy objects, complicated pregnancy, congenital structural features of the vascular pedicle of the kidney and the so-called renal bed.
A complete list of factors for the development of nephroptosis (prolapse of the kidney) includes congenital inferiority of the ligamentous apparatus of the kidney; previous infectious diseases that reduce the activity of mesenchyme and lead to severe changes in connective tissue formations; damage to the ligamentous apparatus of the kidney as a result of injury with complete or partial rupture or separation of the ligaments (fall from a height, sharp blow, severe concussion of the body); significant and rather sharp weight loss with a decrease in the volume of perinephric fiber; weakening of the tone or flabbiness of the anterior abdominal wall with a decrease in intra-abdominal pressure after rapid weight loss, as a result of multiple pregnancies or prolonged labor.
As a rule, nephroptosis (prolapse of the kidney) develops gradually throughout life and is more common in young women, mainly with a slender build.
Symptoms, signs and clinical picture of nephroptosis (prolapse of the kidney).
When a kidney prolapses, it not only moves downwards, but a number of pathological processes occur - rotation (rotation) along its axis, tension of the renal vessels; The blood supply to the kidney deteriorates, the ureter becomes bent, promoting the development of inflammation in the pelvis and the formation of stones. Kidney prolapse (nephroptosis) is manifested by various signs, depending on the stage of nephroptosis. There are 3 stages of nephroptosis:
- at the 1st stage of
kidney prolapse, there are no clinical manifestations, or there are complaints about general changes in well-being and decreased performance, while, as a rule, there is practically no pain. - at the 2nd stage
of kidney prolapse, pain appears in the lumbar region, intensifying in a standing position, sometimes paroxysmal, protein and red blood cells are often detected in the urine. - at the 3rd stage of
nephroptosis, the pain syndrome intensifies, sudden changes in kidney function occur, and performance deteriorates significantly.
Very often, nephroptosis (prolapse of the kidney) goes undiagnosed for a long time and is hidden under the masks of incorrectly established diagnoses - chronic cholecystitis, chronic colitis, chronic adnexitis, acute appendicitis, etc. At the same time, the patient is treated for a long time and unsuccessfully for these ailments, which leads to asthenia and neuroticism of the patient, sharply worsening the quality of life. But the average patient with nephroptosis is a young, slender, thin girl. It is also necessary to remember that the presence of kidney problems affects the course of pregnancy, and the manifestations of nephroptosis during this period only intensify.
“Hand suture in endoscopic surgery”, K. V. Puchkov, D. S. Rodichenko
As a rule, patients seek medical help for the first time with stage 2 nephroptosis. It is characterized by a downward displacement of the kidney by more than 5 cm when the patient moves from a lying position to a standing position and is accompanied by pain in the abdomen or side. In addition, pain with nephroptosis can radiate to the lower abdomen and be accompanied by nausea and chills. Less commonly, pathological mobility of the kidney is manifested by paroxysmal pain such as renal colic (intense bursting, cramping pain), micro- and macrohematuria (admixture of blood in the urine visible to the eye or under microscopy), albuminuria (excessive protein in the urine), and increased blood pressure.
In many cases, patients in whom nephroptosis is accompanied by clinical manifestations are young women of slight build, in whom chronic pain in the lumbar region in an upright position manifests itself as the primary and often the only symptom of nephroptosis. Chronic periodic pain in the side (lower back), a feeling of heaviness, and discomfort in the abdomen are most often observed in a complex manner. The most common complications of nephroptosis are arterial hypertension, kidney infection, urolithiasis and renal colic.
Hypertension develops as a result of kinking of the vessels supplying the kidney, and, as a rule, can lead to the development of arterial crises and a persistent increase in blood pressure.
Read about nephroptosis (prolapse of the kidney), symptoms, diagnosis and treatment methods in the material by K. Puchkov
Rice. 1. Ultrasound of the vessels of the right kidney for stage 3 nephroptosis. in a lying position (left) and standing (right). There is a pronounced change in the diameter of the artery from 7.5 mm to 3.5 mm.
Due to the disruption of the free outflow of urine from the renal pelvis and ureters, with the disturbed position of the kidney and the kinking of the ureters, a local urinary tract infection develops. Urine that is retained in the urinary tract allows bacteria to grow and spread. Symptoms of a urinary tract infection (pyelonephritis and cystitis) include frequent and painful urination, abdominal or lower back pain, fever, and chills. The urine may be cloudy or have an unusual odor.
Urinary stones form from substances found in urine, such as calcium and oxalates. Stagnation of urine in the urinary tract and a decrease in the speed of its free flow into the bladder are predisposing factors for the development of urinary stones. The presence of disorders of urate or purine metabolism sharply increases the likelihood of developing stones in the kidneys or urinary tract. In this case, there is severe pain in the side, back or pelvic pain, blood in the urine, chills and fever, vomiting, burning when urinating.
The presence of a prolapsed kidney sharply increases the risk of injury in case of blunt injuries of the abdomen and pelvis. If the kidney displaced due to nephroptosis is located low in the abdomen or pelvis, then it is more susceptible to injury or blunt trauma.
One of the most common complications of nephroptosis is renal colic. Renal colic when the kidney prolapses is characterized by a painful attack in the side (lumbar region), nausea, chills, tachycardia, oliguria (decreased amount of urine excreted), periodic hematuria (appearance of blood in the urine) or proteinuria (appearance of protein in the urine).
Kidney prolapse consequences
Everything would be fine, but at the same time there is a tension in the vessels feeding the kidney and a bend in the ureter, leading to a disruption of the outflow of urine. As a result, the symptoms (or signs) of nephroptosis are dull pain in the kidney area that appears (or intensifies) after prolonged walking (usually at the end of the day) or physical activity.
Nephroptosis of the kidney is confirmed by the results of excretory urography - an X-ray examination of the kidneys with intravenous administration of a contrast agent. In this case, a “standing” photograph must be taken; it is from this that the stage of nephroptosis (prolapse of the kidney) can be determined.
Diagnosis of nephroptosis (prolapse of the kidney).
Kidney prolapse can be suspected if there is an appropriate clinical picture, as well as if signs of nephroptosis are detected according to ultrasound examination of the kidneys in the supine and standing position. The key diagnostic method, on the basis of which the diagnosis of “pathological mobility of the kidney (nephroptosis)” is established, is intravenous excretory urography with the obligatory performance of one of the images in a standing position, during which a radiopaque substance is injected intravenously and a series of X-ray images of the lumbar region is taken. The diagnosis of nephroptosis cannot be established solely on the basis of ultrasound data; X-ray confirmation of the diagnosis is necessary.
Rice. 2. Ultrasound shows a decrease in the maximum renal blood flow in the right renal artery in a standing position to 70 cm/sec (Fig. on the right) in comparison with these indicators while lying down - 111 cm/sec (Fig. on the left).
Differential diagnosis of pathological mobility of the kidney and its dystopia (congenital malposition of the kidney) is carried out on the basis of ultrasound color Doppler examination with the ability to visualize blood vessels. In this case, an important criterion is the level of origin of the renal artery from the aorta. Color Doppler ultrasound can also measure decreased blood flow in a prolapsed kidney in an upright position.
Also, additional methods for examining the kidneys for nephroptosis are isotope renography and renal scintigraphy.
Kidney prolapse symptoms
Normally, the kidney is kept “in its place” due to a number of mechanisms, among which an important role is played by the fat capsule, which stabilizes the kidney and protects it from external influences.
In people (usually girls) who are naturally slender and/or exhaust themselves with strict diets, the fatty capsule of the kidney becomes thinner, which makes the kidney pathologically mobile. This is manifested by the fact that in a vertical position (or during physical stress) the kidney moves down (sometimes to the level of the pelvis!).
Treatment of nephroptosis (prolapse of the kidney).
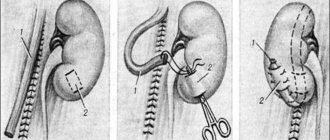
Rice. 3. Puncture sites on the abdominal wall during laparoscopic nephropexy.
Rice. 4. Fixation of the mesh implant to the kidney during laparoscopic surgery.
Rice. 5. Results of laparoscopic nephropexy - data from an excretory urogram in a standing position (10 minutes after administration of a contrast agent). Left before surgery, right 1 month after surgery.
Currently, among the conservative methods of treating a pathologically mobile kidney, the following are used: limiting heavy physical activity of a static nature, wearing a bandage, a complex of physical therapy, high-calorie diets (in order to increase body weight), hydrotherapy (cold compresses, showers, bathing), drug therapy (antibacterial therapy for exacerbation of chronic secondary pyelonephritis, antihypertensive therapy for arterial hypertension). But, unfortunately, these measures help only 10% of patients.
Patients with accidentally detected kidney prolapse should be observed by a urologist and regularly examined: every six months, take urine tests, a biochemical blood test (creatinine, urea, residual nitrogen), perform an ultrasound of the kidneys and bladder, ultrasound of the kidney vessels in a standing and lying position, Perform radioisotope renography per year and, if indicated, intravenous excretory urography. In the absence of negative dynamics, long-term observation is possible.
Indications for surgery to treat nephroptosis occur when the kidney has descended more than 3 vertebral bodies in an upright position of the patient or there is a pronounced clinical picture of kidney prolapse. The operation is indicated if there are signs of decreased blood flow in the renal vessels and impaired excretory function of the kidney, as well as in the case of recurrent urinary infection.
In the last 10–15 years, depending on the chosen surgical approach, the following methods of surgical treatment of nephroptosis are most often used:
- lumbotomy approach is a traditional method of “open” surgery;
- minimally invasive methods of nephropexy (percutaneous, laparoscopic, retroperitoneoscopic, mini-approaches).
The disadvantage of the lumbotomy approach is that it is traumatic - the muscles are widely intersected, the innervation, blood and lymph circulation of the muscles of the lateral abdominal region are disrupted. The rehabilitation period for a patient with an open lumbotomy is long, and the development of postoperative complications (hernia, atony of the abdominal wall, etc.) is possible. The cosmetic effect of the operation is minimal.
Laparoscopic access for nephroptosis has obvious advantages over open operations: less trauma, no blood loss during surgery, good cosmetic results, easier course of the postoperative period, shorter hospital stay, as well as the ability to correct concomitant diseases of the abdominal and pelvic organs that require surgical treatment.
After laparoscopic nephropexy, 96% of patients report positive treatment results - disappearance or significant reduction in pain, normalization of blood pressure, and improvement in urinary passage. When using mesh implants in the treatment of nephroptosis, leading foreign and domestic authors note relapse of the disease in only 0.3% of patients.
The “gold standard” for surgical treatment of nephroptosis is laparoscopic surgery, during which modern, safe mesh implants are used that will reliably hold the kidney in a physiological position. The use of one's own tissue during nephropexy often leads to the development of relapse of nephroptosis and therefore has ceased to be used by leading urologists. The optimal way to use polypropylene meshes is nephropexy with a polypropylene implant at the upper pole.
Watch a video of operations performed by Professor K.V. Puchkov. You can visit the website “Video of operations of the best surgeons in the world.”
Signs of nephroptosis
Mild signs of nephroptosis lead to late diagnosis and difficult treatment. The only symptom that the patient can pay attention to is pain, which is periodic, paroxysmal or nagging in nature. Signs of nephroptosis may be mistaken for manifestations of cholecystitis or acute/chronic appendicitis. At the initial stage of the disease, the symptoms hardly bother the patient, and periodic pain in the lower back and lower abdomen is not paid attention to - they can always be attributed to overwork.
When grade 2 kidney prolapse develops, the pain syndrome becomes more intense, the person may even lose the ability to work, this leads to depression and loss of appetite. Next, urine retention occurs in the kidney, and the result is a significant increase in blood pressure.