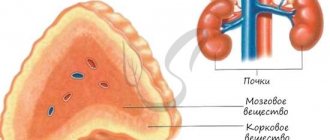
Addison's disease or adrenal insufficiency is a rare endocrine pathology that occurs with equal frequency in both men and women.
The disease is characterized by weight loss, muscle weakness, fatigue, low blood pressure and darkening of the skin. The disease develops when the adrenal glands stop producing enough of the hormone cortisol, and in some cases, the hormone aldosterone. For this reason, the disease is called chronic adrenal insufficiency.
Impaired cortisol secretion, or adrenal insufficiency, develops for various reasons. The disease may be associated with dysfunction of the adrenal glands (primary adrenal insufficiency) or insufficient secretion of ACTH from the pituitary gland (secondary adrenal insufficiency).
What are the signs and symptoms of adrenal insufficiency?
Clinical signs of adrenal insufficiency usually develop gradually. General symptoms of the disease:
- Chronic fatigue that gradually increases.
- Muscle weakness.
- Loss of appetite.
- Weight loss.
- Low blood pressure, which drops significantly when changing body position; with a sharp rise, dizziness or fainting occurs.
- Irritability.
- Depression.
- Low blood sugar (hypoglycemia), including sweating, nausea, rapid heartbeat, and anxiety due to hypoglycemia.
- Craving for salty foods.
- Irregular menstruation.
In 50% of cases there are:
- Nausea.
- Vomit.
- Diarrhea.
Skin changes are also pronounced in Addisson's disease.
Characteristic areas of hyperpigmentation in the form of a dark tan, covering large areas of the body, including areas of skin on non-exposed parts of the body. Darkening of the skin is most noticeable in scar areas, skin folds, elbows, knees, fingers and toes, lips and mucous membranes.
As a result of mineralocorticoid deficiency and significant loss of salt, cravings for salty foods are observed, which is also a characteristic symptom of the disease.
Because symptoms progress slowly, they are usually ignored by patients until a stressful event occurs, when an illness or accident leads to decompensation of the disease and a keratinous condition. This is called Addisonian crisis, or acute adrenal insufficiency. 25 percent of patients first develop symptoms during Addisonian crisis.
Symptoms of a crisis include sudden stabbing pain in the lower back, abdomen and legs, severe vomiting and diarrhea, severe dehydration, low blood pressure accompanied by loss of consciousness.
Acute adrenal insufficiency
Acute adrenal insufficiency
Professor Karpov Vladimir Vladimirovich - Doctor of Medical Sciences, pediatrician of the highest qualification, head of the department of childhood diseases of Rostov State Medical University, author of various methods and scientific works.
Professor Chepurnaya Maria Mikhailovna - Doctor of Medical Sciences, Honored Doctor of the Russian Federation, Head of the Pulmonology Department of the Regional Children's Hospital, Rostov-on-Don
Andriyashchenko Irina Ivanovna is a pediatrician of the highest qualification category.
Elizaveta Andreevna Turbeeva – page editor
Acute adrenal insufficiency
Book: “Pathological syndromes in pediatrics.” (Lukyanova E.M.)
The disease is characterized by dysfunction of the adrenal cortex. However, in severe processes accompanied by damage to the cortical and medulla layers of the adrenal glands, their total failure may occur.
Acute insufficiency most often occurs under various stress conditions in children with latent pre-existing hypofunction of the adrenal cortex. It can also be observed in the so-called thymicolymphatic status.
Acute adrenal insufficiency is caused mainly by an infectious process. The most common cause of adrenal insufficiency today is meningococcal infection. However, the same damage to this organ can develop with toxic diphtheria, severe influenza, strepto-, staphylococcal toxic-septic processes, with intestinal infections occurring with toxicosis.
In newborns, the cause of acute adrenal insufficiency can be acute hemorrhage (more often in premature infants) due to birth trauma or asphyxia. Very rarely, the cause of adrenal insufficiency is surgical or household trauma in children of different ages.
Finally, acute adrenal insufficiency can result from improper administration of hormonal therapy. What is important is the sudden withdrawal of large doses of corticosteroids prescribed for a long time, which leads to inhibition of the production of one’s own hormones.
In practice, when a doctor encounters an acute adrenal insufficiency syndrome, the first thing to think about is meningococcemia and the developing damage to the adrenal glands against this background.
The pathogenesis of the complication involves a chain of sequentially developing processes. Bacterial exo- and endotoxins sensitize the body, damage blood vessels, and disrupt the blood coagulation system. Against this background, thrombovasculitis develops (mainly in small vessels) with microcirculation disorders, which is confirmed by our research data.
During capillaroscopy in children, sharp changes in blood flow are observed - stagnation, intermittent blood flow, stasis in dilated vessels. These disorders, apparently, as a result of the action of toxins on the vascular system, contribute to the development of thrombovasculitis. The latter lead to the appearance of infarct-like areas of tissue necrosis. In parallel, through the affected vascular wall, red blood cells are released into the surrounding tissues through diathesis.
The hemorrhagic component is added to the necrotic component. They can be found in various tissue areas (skin and internal organs) in various relationships. Therefore, along with hemorrhagic (mostly small and superficial) elements, necrotic (larger and deeper) elements are also noted.
Necrotic tissue undergoes resorption. Toxic products are formed in foci of necrosis. Autotoxins aggravate the effect of microbial toxins on the body. Acute intoxication occurs with dysfunction of a number of organs. A similar process can unfold in the adrenal glands.
With small necrotic areas at the site of thrombosis, edema and hemorrhage develop, significantly impairing the function of both the medulla and the cortical layer of the organ. However, such insufficiency may be transient and goes away especially easily and quickly with early treatment.
With extensive areas of necrosis of adrenal tissue, a complete loss of their gluco- and mineralocorticoid, as well as sympathetic-adrenal function occurs, which leads to severe dysfunction of many organs.
Thus, loss of corticosteroid function makes the body defenseless, since adrenal hormones are needed to develop a protective adaptation syndrome in stressful situations. It is well known that adrenaline and norepinephrine provide vasomotor and trophic innervation of organs.
They play an important role in increasing the performance of organs, which is especially important and necessary in severe diseases, when the body mobilizes all its strength to fight the damage that has occurred. At the same time, steroid hormones, supporting intensive metabolism in the cells of the body, create a favorable background and conditions for an enhanced cell reaction to the action of sympathetic-adrenal substances.
As a result, the efficiency of organs increases. In case of dysfunction of the adrenal glands, a sharp drop in blood pressure occurs due to the loss of the vasoconstrictive effect of the sympathetic nerves on the argerioles, slowing down and weakening of heart contractions. Collapse develops. Hypotension and adynamia are noted.
Water-salt metabolism is disrupted. As the process progresses and there is no treatment, the patient dies with the development of adrenal coma and severe collapse.
Life experience shows that, based on one clinical picture of the disease, it is often difficult or even impossible to determine the depth and prevalence of the pathological process. An important rule follows from this: immediately begin intensive therapy for all persons with acute adrenal insufficiency, regardless of the clinical severity of the process.
In this way, it is often possible to save seemingly hopeless patients. During a pathological examination of those killed from acute adrenal insufficiency, massive necrosis with hemorrhages and edema is found in the adrenal tissue.
With influenza and severe intestinal infections (toxic dysentery, etc.), accompanied by adrenal insufficiency, pinpoint hemorrhages are detected on the skin, and less often on the mucous membranes. Areas of massive necrosis (especially with meningococcemia) can be found on the skin, mucous membranes and many internal organs.
Clinic for meningococcemia (Waterhouse-Friderichsen syndrome). The disease begins acutely, with a rise in temperature, often to high numbers (39-41°). Pronounced anxiety appears. Older children complain of headaches, dizziness, pain in the abdomen and limbs, and therefore the disease is often mistaken for the flu.
As the disease progresses, anxiety gives way to lethargy, adynamia, lethargy, then complete loss of consciousness and the development of a coma. Relatively soon after the onset of the disease, elements of a meningococcemic rash appear on the skin, characterized by great polymorphism.
They vary in size (from 1-2 mm to 5-6 cm in diameter), brightness (expressiveness), shape, which creates a motley picture reminiscent of a starry sky. The number of elements varies in different patients (from 2-4 to many).
Most elements have an irregular shape with large (more than 2 mm) elements having processes, which are affected and thrombosed vessels visible through the skin with infiltration around the erythrocytes released through diapedesis.
The color of the elements ranges from pink-red, cherry-red to dark cherry. Most large elements (more than 2-3 mm) are necrotic areas of tissue. However, very often, spots of hyperemia appear around clearly necrotic elements, reminiscent of surface skin changes contaminated with paint.
Soon after the onset of the disease, signs of collapse appear. Blood pressure drops, at first slightly, and then to critical numbers and below, and sometimes to zero (not determined). Purple-bluish spots appear on the skin of the torso, limbs, scrotum and ears.
The pulse is thready, heart sounds are muffled, arrhythmia. Necrotic elements usually increase in size and quantity and merge. Necrosis of large areas of tissue of the fingers and toes, heels, tip of the nose, and in rare cases, even the distal parts of the extremities may occur. In place of necrotic areas, bluish blisters filled with clear liquid form.
Subsequently, breathing disorder appears, it becomes arrhythmic, superficial, irregular, rapid, and then toxic, like Cheyne-Stokes. Diuresis is impaired, oliguria is observed, and then anuria. In cases of severe toxicosis, collapse and coma, the patient dies.
Our observations have shown that meningococcemia without involvement of the meninges almost never occurs, although many children do not have obvious signs of their damage - meningeal signs, which is especially often noted with severe intoxication. Lumbar puncture often reveals purulent cerebrospinal fluid. In some children, the cerebrospinal fluid is serous, but with a predominance of neutrophils.
During the fulminant course of meningococcemia with adrenal insufficiency, we observed very small changes in the cerebrospinal fluid - pleocytosis of 16-20 cells (but all neutrophils!), a positive Pandi reaction with normal protein content in the cerebrospinal fluid.
At the same time, a huge number of meningococci were noted. In connection with the above, we believe that if meningococcemia is suspected (including those accompanied by adrenal insufficiency), it is necessary to perform a lumbar puncture with a cerebrospinal fluid analysis.
In the blood of meningococcemia with adrenal insufficiency, changes typical for sepsis are revealed - pronounced leukocytosis (20,000-30,000 in 1 mm), sharp neutrophilia with a large shift to the left to stabs (20-40%), less often - to young, promyelocytes and even myelocytes, significantly increased ESR (35-60 mm per hour or more).
However, with the galloping course of the disease, changes in the blood do not have time to develop and can only be reduced to severe neutrophilia, sometimes with a shift of the formula to the left without other changes. Microscopic examination can detect meningococci.
Damage to the adrenal glands is observed in toxic, hemorrhagic and gangrenous forms of diphtheria. In this case, hyperemia and numerous hemorrhages in the adrenal glands usually develop. If the patient does not die in the first 2-3 days, then extensive necrosis of adrenal tissue may occur.
Clinic. Symptoms of adrenal gland damage are superimposed on the symptoms of toxic diphtheria. The extreme severity of the condition, adynamia, lethargy and symptoms of collapse come to the fore: a weak, thread-like pulse, a sharp drop in blood pressure (may not be detected). Marbling of the skin and petechial hemorrhages and dullness of heart sounds appear. Oliguria, anuria. With such phenomena, the patient dies.
The adrenal glands are often affected by the flu. According to our data, adrenal gland damage occurs in 3-6% of deaths in such children.
In the clinical picture of the disease, against the background of severe intoxication, hyperthermia and typical flu symptoms (aches throughout the body, pain in the eyes and headache, damage to the mucous membrane of the pharynx, feverish blush of the cheeks), lethargy and adynamia appear. There is a moderate amount of petechial hemorrhages on the skin and mucous membranes.
Clinical symptoms of collapse develop relatively quickly: thready pulse, drop in blood pressure. Marbling of the skin appears, which is associated with stasis and paretic dilation of capillaries and small vessels. Since the toxic form of influenza causes damage to the heart muscle, kidneys, and central nervous system, symptoms of myocarditis, meningoencephalitis, and toxic kidney damage may occur.
Transient adrenal insufficiency can occur in infants with toxicoses and toxic-septic conditions of various etiologies. The disease in such cases is accompanied by lethargy, toxicosis, exicosis and takes a protracted course, despite ongoing detoxification and antibacterial therapy.
WL Deemer and N. Silver (1955) believe that in all patients with a toxic condition and exicosis that is not amenable to dehydration therapy, one should think about adrenal insufficiency. This dictates the prescription of steroid therapy necessary for adrenal insufficiency.
Acute adrenal insufficiency in newborns develops as a result of hemorrhage into the adrenal glands during asphyxia and birth trauma, against the background of a viral infection, pneumonia, sepsis and other diseases, with congenital defects in the development of the adrenal glands.
The clinical picture resembles Waterhouse-Friderichsen syndrome. The condition of the newborn is serious, the child is adynamic, there is severe lethargy, muscle hypotonia, hypo- or areflexia, pallor of the skin, drop in blood pressure, weakness of cardiac activity, thread-like pulse, cold extremities.
Possible regurgitation and vomiting, petechial elements on the skin. On palpation, moderate abdominal tension can be noted; enlarged adrenal glands can often be palpated. Sometimes there are attacks of clonic and clonic-tonic convulsions, hyperthermia.
This condition can be observed in the child from the moment of birth or develop several hours after it. Diagnosis and differential diagnosis. Timely recognition of adrenal lesions is of paramount importance for modern therapy.
However, for rational treatment it is necessary not only to establish a diagnosis of adrenal insufficiency, but also to clarify the etiology of the disease. Only in this case will the doctor be able to prescribe, in addition to pathogenetic etiotropic therapy, necessary in order to interrupt the progression of the process in the adrenal glands. Clarifying the epidemic history and taking into account the clinical symptoms of the disease, against which the adrenal glands develop, helps to clarify the etiology of the disease.
The diagnosis of acute adrenal insufficiency in children with meningococcal infection is established taking into account indications of the child’s contact 2-10 days before the disease with a patient with a typical generalized form of meningococcal infection (meningococcemia, meningitis) or a carrier of meningococcus in the group.
All children with whom the sick child was in contact are tested for meningococcal discharge from the throat and nose immediately after a suspicion of meningococcal infection arises. This sometimes allows a correct diagnosis to be made on the first day of the disease.
The progressive course of the disease with a typical skin rash (hemorrhagic-necrotic rash of irregular shape, of various sizes with process elements located asymmetrically), a drop in blood pressure and other symptoms of collapse, septic changes in the blood is taken into account
A lumbar puncture with cerebrospinal fluid analysis is required. The presence of meningeal syndrome, changes in blood and cerebrospinal fluid in a typical rash allows one to correctly determine the etiological nature of the disease even before meningococcus is detected.
This is extremely important, since currently meningococcus is not always cultured even in large laboratories. Cultures of mucus from the throat and nose for meningococcal flora should also be used, although these tests are often negative. Meningococcus is cultured from the cerebrospinal fluid ten or more times more often.
The diagnosis of toxic diphtheria of the pharynx is established on the basis of epidemic history and typical symptoms of diphtheria. Severe pallor of the skin, intoxication, swelling of the tissue of the neck, sometimes descending to the chest, swelling of the tonsils and surrounding tissue, sometimes reaching such an extent that the tonsils are in contact with each other (the pharynx is blocked).
On the mucous membrane of the tonsils, and sometimes the soft palate and uvula, whitish-gray shiny smooth plaques (plus tissue) are visible that cannot be removed with a spatula. Symptoms of myocarditis, nephritis, and damage to the nervous system (paresis, paralysis) are detected. A toxigenic strain of diphtheria bacillus (usually the gravis type) is found in a throat smear.
Against this background, a typical vascular syndrome of adrenal insufficiency (collapse) develops. The latter should be distinguished from myocarditis with signs of heart failure, in which there is a sharp shift in the boundaries of the heart and an increase in its size, dullness of sounds, arrhythmias, swelling in the legs, an increase in the size of the liver, pronounced changes in the electrocardiogram with a decrease in the functional state of the heart muscle.
With adrenal insufficiency, changes in the heart muscle are moderately pronounced, symptoms of vascular insufficiency predominate (a sharp drop in blood pressure, a frequent thread-like pulse, an increase in signs of adynamia). Very rarely, a doctor may encounter a combination of myocarditis and adrenal insufficiency.
The diagnosis of influenza is made on the basis of the acute onset of the disease with high fever, pronounced hyperemia of the mucous membrane of the pharynx with a predominance of symptoms of intoxication, petechial hemorrhages on the skin and mucous membrane of the pharynx and cheeks, severe condition, typical complaints (aches in the whole body, pain in the eyeballs, headache pain, weakness). Leukopenia and lymphocytosis are observed in the blood.
There are no changes in the cerebrospinal fluid, and in cases of influenza with damage to the nervous system, lymphocytic pleocytosis is detected with normal or slightly increased protein content. Elements of the rash with influenza do not exceed 2-5 mm in diameter and are not necrotic in nature.
The petechial rash that occurs with influenza never occurs with severe adrenal insufficiency in patients with meningococcemia. Often there is a need to carry out a differential diagnosis of the latter with a number of somatic diseases that occur with a hemorrhagic rash: hemorrhagic vasculitis, Werlhof's disease, leukemia (Table 1).
So. Hemorrhagic vasculitis (Schönlein-Henoch disease, capillary toxicosis) is characterized by a petechial-papular rash with symmetrically located elements (resembling round spots in shape) around the joints, on the feet, legs, buttocks, differing only in size (no more than 1-4 mm in diameter), renal and intestinal bleeding in the absence of septic blood and signs of damage to the meninges (including changes in the cerebrospinal fluid). Massive hemorrhages and bruises in the absence of meningeal signs, the presence of thrombocytopenia indicate the presence of thrombocytopenic purpura in the patient.
Leukemia is also characterized by elements such as hemorrhages (from petechial to large bruises). There is an increase (systemic) in the size of the lymph nodes, liver and spleen and typical blood changes.
The experience of the neuroinfectious department of the pediatric infections clinic of the Kyiv Medical Institute shows that a comprehensive examination of patients, taking into account these auxiliary research methods, helps to establish the diagnosis of adrenal insufficiency in meningococcal infection already in the early stages of the disease.
In cases that are particularly difficult to recognize, if there is a suspicion of adrenal insufficiency of meningococcal etiology, it is necessary to immediately begin etiotropic therapy. This is less dangerous for the patient than delaying treatment if the diagnosis is subsequently confirmed.
Delayed therapy for meningococcal infection with adrenal insufficiency is almost ineffective, and the disease ends in death.
Establishing adrenal insufficiency in newborns is very difficult. However, if the doctor remembers such a pathology, especially in severe cases of childbirth (intrauterine asphyxia, provision of benefits during delivery, in the presence of birth trauma), the appearance of collapse in the child, a sudden sharp deterioration in the general condition help to make the correct diagnosis.
The course and outcome of adrenal insufficiency depends on the timeliness of treatment measures, their correct implementation, on the severity and depth of adrenal lesions. However, the mortality rate in this pathology remains high, which is most often associated with late diagnosis and late prescription of pathogenetic therapy.
With timely treatment, the condition improves relatively quickly; by the end of the day, adynamia, lethargy and intoxication decrease; consciousness clears up; blood pressure rises; pulse improves; temperature drops; symptoms of collapse disappear. Elements of the rash, caused by tissue necrosis, shrink into a crust that takes on a dark cherry-black color. The latter is subsequently rejected, and epithelization of the wound occurs. At
Acute adrenal insufficiency
Acute adrenal insufficiency
In the presence of large elements, scarring occurs. Blood pressure, blood and cerebrospinal fluid gradually normalize. Full recovery ensues.
Treatment of adrenal insufficiency in meningococcemia. A patient with meningococcemia, and especially with adrenal insufficiency, should be immediately admitted to the nearest hospital, since transportation to a special institution (an infectious diseases hospital or a neuroinfectious department) sometimes takes a long time, is tedious and can be fatal for him.
Minutes, not just hours, play a role in the treatment of this disease. If you delay, valuable time for effective therapy may be lost.
The patient is prescribed pathogenetic treatment taking into account developing disorders. Antibacterial therapy. The most effective is the potassium salt of benzylpenicillin, which is used at a dose of 200,000-500,000 units per kg of body weight per day intramuscularly.
Such large doses are prescribed because benzylpenicillin penetrates the subarachnoid space in low concentrations (1/20-1/30 of its concentration in the blood).
The individual dose of the drug is directly proportional to the severity of the condition and the length of time that has passed since the day of illness, and inversely proportional to the age of the sick child.
The daily dose of benzylpenicillin is divided into 8-12 injections. It should be borne in mind that when administering large doses of benzylpenicillin, it is necessary to take into account the sodium or potassium salts introduced with it.
The use of a large dose of benzylpenicillin potassium salt can lead to an increase in potassium in the body. Therefore, the sodium and potassium salts of the drug should be administered alternately.
Currently, it is not recommended to administer sulfonamides in parallel with benzylpenicillin, since they inhibit cell division, which reduces the effectiveness of benzylpenicillin (V.I. Pokrovsky and Yu.A. Vengerov, 1973).
Streptomycin in the usual dosage when administered intramuscularly does not penetrate well into the subarachnoid space. Large doses have a toxic effect on the auditory nerve. Therefore, its use is very often contraindicated.
For a patient who is in a very serious condition, especially with symptoms of intoxication, late admission and suspicion of another infection (staphylococcal, streptococcal, pneumococcal), or admitted with a relapse of meningitis, it is more logical to prescribe a broader-spectrum antibiotic from the very beginning.
According to observations from our clinic, intramuscular administration of chloramphenicol sodium succinate (50,000 - 80,000 units per 1 kg of body weight per day), or chlorocide, is very effective. From 30 to 100 mg/kg per day in four injections. In rare cases of sensitization of the body to penicillin, tetraolean, gentamicin, rifamycin are prescribed intravenously or intramuscularly in maximum therapeutic doses. If there is no effect from the treatment within 3-4 days, antibiotics should be changed.
For the purpose of detoxification therapy, drip administration of Ringer's solution or isotopic sodium chloride solution and 5% glucose solution (500-600 ml of each) is prescribed. Hemodez (syn. neocompansan) is prescribed in an amount of 100-300 ml, plasma or albumin intravenously (60-100 ml).
Corticosteroid therapy is replacement therapy. It is prescribed immediately after diagnosis (the sooner the better!) and even if this disease is suspected.
Hydrocortisone hemisuccinate is used at a dose of 10-25 mg/kg body weight in parallel with prednisolone hydrochloride 3-5 mg/kg body weight intravenously until blood pressure rises (subcutaneous administration of the drug is ineffective!), then switch to drip administration and reduce the dose by half. At the same time, DOXA (5-8 mg) is administered intramuscularly.
To raise blood pressure, polyglucin or rheopolyglucin (200-600 ml) is prescribed intravenously. If there is no effect, 0.5-1 ml of a 5% solution of ephedrine hydrochloride is administered intravenously. If necessary, this dose can be repeated.
To enhance the removal of fluid from the body, that is, to enhance the detoxification effect, 1-1.5 ml of a 10-20% solution of mannitol or furosemide (syn. Lasix) is prescribed intravenously. It should be remembered that mannitol solution cannot be mixed in a dropper with other solutions, as this reduces the concentration of the drug and may negate its effect.
Vitamin therapy. 2-8 ml of a 5% solution of vitamin C is prescribed intravenously along with 50-100 mg of cocarbokeylase. At the same time, the patient takes multivitamins orally.
Cardiac glycosides - strophanthin (0.05% solution 0.1 - 0.35 ml) or korglykon (0.15-0.75 ml) - are prescribed only after blood pressure has been restored. Strophanthin should not be administered together with vitamin C, since the acidic environment neutralizes strophanthin.
Effect on the blood coagulation system. Heparin and fibrinolysin 3000-5000 units are administered intravenously if the patient was admitted no later than 1-3 days from the onset of the disease (one or two days in a row).
For hyperthermia, amidopyrine, intramuscular analgin, physical cooling methods are prescribed: a bottle of cold water on the area of large vessels (temperature - 10-15 °), hang an ice pack over the head, wipe the body with a vinegar solution (1 teaspoon per 1 liter of water), use the fan less often. Craniocerebral hypothermia can be used.
Resuscitation measures - closed cardiac massage and artificial respiration (mouth to mouth or controlled breathing) are carried out in case of severe impairment of respiratory function and asystole.
To stop seizures, GHB (sodium hydroxybutyrate at a dose of 70-120 mg/kg body weight, can be repeated after 5 hours, that is, after the drug is removed from the body) or chloral hydrate in an enema (1.5-2% solution - 20-30 ml) is administered drip-wise ).
It is advisable to correct the electrolyte composition of the blood taking into account existing disorders. Hypokalemia is more common, and therefore a solution of potassium chloride (4%—30—100 ml) is administered intravenously.
Recently, to prevent progressive tissue necrosis, an irothease inhibitor, trazylol (syn. contrical, tsalol) 25,000-50,000 units, has been used. per day intravenously drip. The drug is diluted in a 5% glucose solution or isotonic sodium chloride solution (2-3 days in a row).
Diet therapy. In extremely severe conditions, if the patient does not swallow, parenteral nutrition is used or he is fed through a tube with liquid food - acidophilus-yeast milk with paste or kefir with cottage cheese (mashed), then liquid vegetable soup in meat broth, pureed meat is prescribed.
After the condition improves, split meals with a gradual transition to a normal diet (with an increase in calories and an expansion of the composition of food ingredients). It is advisable to introduce sour milk mixtures (kefir, acidophilus-yeast milk) into food, which prevents the development of dysbacteriosis, vegetable dishes, fruits, juices to replenish the body with salts and natural vitamins.
Stimulating therapy involves the administration of blood and its substitutes, as well as blood products (plasma, gamma globulin), which is carried out after the acute process has subsided and the function of the excretory organs has been restored if indicated (prolonged recovery).
Intensive transfusion drip therapy is carried out for 2-4 days until there is a clear improvement in the general condition and function of organs. Sometimes renal failure develops after this, which requires hemodialysis and appropriate dietary and drug therapy.
Antibiotics are prescribed until the temperature, blood and cerebrospinal fluid tests normalize (on average 7-10 days). Treatment of adrenal insufficiency of other etiologies. Regardless of the etiology of the disease, when adrenal insufficiency manifests itself, replacement therapy with corticosteroids, which are listed above, is necessary.
In case of adrenal insufficiency of diphtheria etiology, broad-spectrum antibiotics are used in the usual dosage; anti-diphtheria serum according to Bezredka is necessarily administered in the amount of 50,000–80,000 units (repeatedly). Strychnine is prescribed to tonify the heart muscle (0.1% solution—1-3 ml, no more than 5 ml, and the drug is not prescribed to children under 2 years of age!).
In case of influenza etiology of the disease, anti-influenza gamma globulin (4-6 doses) is administered repeatedly along with first symptomatic therapy.
For hemorrhage in the adrenal glands in newborns, a gentle regimen is prescribed. The child should be swaddled carefully, washed and fed in the crib, shifted extremely carefully, along with the urgent administration of hormones, ascorutin, calcium chloride, vitamin PP and folic acid, vikasol, and, if indicated, aminocaproic acid are prescribed.
Intravenous administration of saline solutions, taking into account sodium and potassium levels, and cardiac medications are required. In case of adrenal insufficiency that has developed during the abolition of massive or long-term steroid therapy, replacement therapy with corticosteroids is urgently prescribed until the syndrome is eliminated; At the same time, the usual doses of antibiotics and other therapy are prescribed.
Timely and correctly administered treatment with reversibility of the process in the adrenal glands allows for recovery in most children with adrenal insufficiency.
OPT ET 02/21/2016
Diagnosis of the disease
At an early stage of the disease, adrenal insufficiency is difficult to diagnose. Only dark tanned skin attracts attention, which may be a reason to suspect Addison's disease.
Biochemical blood parameters are determined to determine insufficient levels of cortisol, aldosterone and ACTH. The adrenal glands and pituitary gland are examined X-ray and NMR, which helps to establish the cause of the disease.
A pharmacological test with ACTH is performed. This is the most specific test for diagnosing the disease.
In the absence of timely treatment of the disease, a severe Addisonian crisis develops, the outcome of which can be fatal.
ONLINE REGISTRATION at the DIANA clinic
You can make an appointment by calling the toll-free phone number 8-800-707-15-60 or filling out the contact form. In this case, we will contact you ourselves.
If you find an error, please select a piece of text and press Ctrl+Enter
Causes
Acute adrenal insufficiency most often occurs in patients with chronic adrenal insufficiency.
For example, if they stop taking corticosteroid hormones to compensate for the lack of their own. The same can happen against the background of injuries, operations, acute infectious diseases, climate change, heavy physical activity, and severe psycho-emotional stress. In addition, Addisonian crisis occurs:
- with acute hemorrhage in the adrenal glands or with the development of infarction (tissue necrosis);
- for meningitis, sepsis, severe blood loss (wounds, childbirth), burn disease.
Signs in women
One of the very first manifestations of hypocortisolism is a feeling of constant weakness. At first, sleep and rest reduce it, but as it progresses, patients wake up in the morning sleep-deprived and feel the need for stimulants - coffee, strong tea, energy drinks, which give a short-term burst of strength. At night, I usually experience insomnia, anxiety, and nightmares. Sleep becomes intermittent and shallow.
The following symptoms are typical:
- depressed mood background;
- low pressure;
- headache, dizziness;
- loss of appetite, alternating with sudden attacks of hunger, a tendency to salty, sweet, spicy foods;
- darkening of the eyes with a sudden change in body position;
- nausea, abdominal pain, unstable stool;
- disruption of the menstrual cycle;
- frequent colds, prolonged infections, transition to chronic forms;
- intolerance to medications or foods, allergic reactions;
- constant anxiety, irritability;
- memory loss, difficulty concentrating.
Intermittent and shallow sleep