Description of drugs in Lesson No. 07
Description of drugs in Pathological Anatomy in Lesson No. 7
(This is an indicative description, not a cathedral one, some drugs may be missing, as is the description of previous years)
- LESSON No. 7
Inflammation. Acute inflammation. Morphology of exudative inflammation.
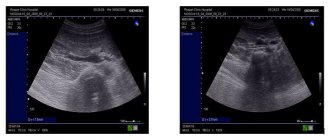
Macrodrug of embolic purulent nephritis.
The size of the kidney is increased, the consistency is flabby, there are many areas (abscesses) in the lesion, after opening which a cavity remains.
Microslide No. 42. Embolic purulent nephritis.
Multiple accumulations of neutrophils (abscesses) are observed in the cortex and medulla; the tissue in the foci is lysed. In the center of the lesions there are small vessels obstructed by small emboli. Around the foci of inflammation, the vessels are obstructed and full of blood.
Macropreparation of cerebrospinal purulent leptomeningitis.
The soft meninges are thickened, they are dull, saturated with a thick greenish-yellow mass of pus, the furrows and convolutions are smoothed. Changes affect the surface of the frontal and parietal lobes.
Microslide No. 95. Cerebrospinal purulent meningitis.
In the soft meninges, neutrophilic infiltration is observed, the foci of which are located diffusely. The vessels are full of blood. In the brain substance there are signs of perivascular and pericellular inflammation.
Macrodrug of fibrous pericarditis (“hairy heart”).
The pericardium is thickened, gray, covered with thin gray fibrin threads. It often appears above the infarction area.
Macrodrug of diphtheritic colitis.
The intestinal wall is thickened, the mucous membrane is necrotic and partially replaced by a yellowish film. The film is dense, tightly fused to the adjacent tissues, and when you try to tear it off, ulcers form.
Microslide No. 131. Diphtheritic colitis.
The mucosa and submucosa are necrotic and represent a homogeneous pink mass. Directly below it is the muscular layer. Grayish films fused to it extend from the edge of the mucosa.
Microslide No. 39. Lobar pneumonia.
The preparation shows that all alveoli are involved in the inflammatory process, in the lumen of which there is pink exudate and leukocytes.
With additional staining for fibrin according to Shueninov, purple fibrin threads are visible, in places penetrating through the pores in the alveolar walls.
Macrodrug of post-catarrhal gastritis.
The folds of the stomach are enlarged, the vessels are dilated, full of blood, a large amount of exudate is visible on the folds.
APOSTEMATOUS NEPHRITIS
Accent placement: APOSTEMATIC JADEAPOSTEMATOUS NEPHRITIS (Late Latin apostematosus, from the Greek apostema abscess, abscess; synonym pustular nephritis) is a metastatic suppurative process in the kidney, manifested by the formation of many pustules, mainly in its cortical substance. A. n. - one of the forms of acute pyelonephritis; occurs in 36% of patients with acute pyelonephritis. Among patients with kidney diseases treated in urological hospitals, A. n. observed in 4.5% of cases.
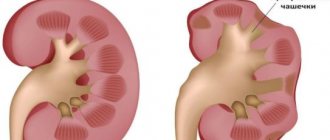
Rice. 1. Multiple rashes on the posterior surface of the kidney. Reactive thickening and infiltration of perirenal fatty tissue
Rice. 2. The same kidney on a section: pustules are located mainly in the cortex
Etiology. The infection enters the kidney through the hematogenous, lymphohematogenous route. If it is brought in from a source of purulent infection located far from the kidney and urinary tract, then the causative agents of inflammation are usually gram-positive cocci, mainly staphylococci. When the infection is primarily localized in the urinary tract, E. coli, Proteus, Pseudomonas aeruginosa, etc. more often enter the kidney. Secondary A. n.
With obstruction of the urinary tract A. n. is predominantly one-sided; with septicopyemia (see Sepsis
) both kidneys are often affected.
Pathological anatomy
. In 24% of cases A. n. combined with kidney carbuncle. These two types of purulent lesions of the night represent a pathogenetically single process, revealed only in different sequences and intensity of its development. For A. n. characterized by the presence of multiple small abscesses, mainly in the cortex; for a kidney carbuncle - the presence of a localized suppurative process, characterized by a tumor-like progressive growth of inflammatory infiltration without a tendency to further abscess formation.
With A. n. the bud is enlarged, gray-cherry in color. The perinephric tissue is edematous. Upon removal of the fibrous capsule from the kidney, multiple small abscesses, ranging in size from a pinhead to a pea, located singly or in groups, are visible. On a section of the kidney, small abscesses are found in the medulla (print table, volume 1, article 472, Fig. 1 and 2). Microscopically multiple foci of purulent inflammation in the interstitial tissue. Around the Malpighian glomeruli there are accumulations of small cell infiltrates with foci of necrosis. The urinary tubules are compressed by perivascular infiltrates.
Pathogenesis
. Development of A. science a number of factors are favorable: previous diseases of the urinary organs, weakening of the body's defenses, urodynamic disorders affecting the passage of urine, the presence of dysplastic foci in the renal tissue, congenital immaturity of the nephropes. Impaired patency of the urinary tract is most often caused by the presence of stones in them, narrowing of their lumen, or prostate adenoma.
The infection, having penetrated the kidney, is first localized in the interstitial tissue. With the so-called In the urinogenic route of infection, microorganisms from the genitourinary organs penetrate through the venous or lymphatic channel into the blood, and then enter the interstitium of the kidney. In addition, infection can penetrate from the collecting system into the interstitial tissue during pyelorenal reflux.
Microbes settle in the venous peritubular capillaries and then penetrate the interstitium, where they cause the formation of foci of inflammation. From here, inflammatory infiltrates spread through the interstitial tissue of the perivenous spaces, emerging on the surface of the kidney, into the subcapsular fissures, according to the location of the stellate veins. Subsequently, pus and bacteria penetrate into the lumen of the tubules. Embolic glomerulitis with A. n. - a secondary phenomenon.
During the recovery phase, granulation tissue forms at the sites of pustules, which then scars.
Clinical picture
. A. n. observed at any age, somewhat more often in women. Unilateral process occurs in 96.6%, bilateral - in 3.4% of patients. The clinical picture consists of signs typical of a general severe infectious process with deep intoxication: headache
pain, general malaise, high fever of constant or remitting type, chills. Sometimes these phenomena are expressed so intensely that they give reason to suspect an acute infectious disease. After some time, local symptoms appear: pain in the lumbar region, radiating to the upper abdomen, shoulder, along the ureter or to the thigh. A. n. may be accompanied by bacteremic shock: a sharp deterioration in general condition, pallor of the skin, acrotsnanosis, weak pulse, drop in blood pressure, rapid breathing.
On palpation, pain in the area of the affected kidney, muscle tension in the lumbar region and abdominal wall are determined. Sharp pain in the area of the costovertebral angle is often noted.
Important signs of a purulent process in the kidney are pyuria and bacteriuria. In the initial stage of A. n. There may not be any changes in the urine, since cortically located abscesses only sometimes break into the renal pelvis. Later, erythrocytes, leukocytes, slight albuminuria and microhematuria, bacteriuria appear in the urine (in 85% of patients found in 1 ml
urine more than 100 thousand bacteria).
In the blood there is often pronounced leukocytosis with significant neutrophilia.
Complications. The most common complication of A. n. - paranephritis
(cm.).
The most dangerous complication of A. n. is septicopyemia, which can also affect the other kidney. When the process is localized in the upper pole of the kidney, a subphrenic abscess and reactive pleurisy may occur, and when localized in the lower pole, a picture of psoitis can occur. In cases where abscesses are located predominantly on the anterior surface of the kidney, peritoneal phenomena and sometimes a picture of an acute abdomen are observed. A. n. may also be complicated by phlegmon of the retroperitoneal tissue.
Diagnosis
is established on the basis of the clinical picture of the disease and special research methods.
In recognizing the side of the lesion, a certain assistance is provided by the so-called. comparative leukocytosis: the number of leukocytes in blood taken from the skin of the lumbar region on the side of the affected kidney is greater than in blood taken from the skin of the lumbar region of the opposite healthy side and from a finger. A new method of research and diagnosis is being used - color thermography of the skin of the lumbar areas. Thermography is based on the ability of cholesteric liquid crystals to change their color in response to the slightest local fluctuations in body temperature. Thanks to this method, it is possible to establish and clarify the localization of the inflammatory process in the kidneys (see Thermography
).
With A. n. There are the following radiological signs: an increase in the size of the kidney in 80% of patients, scoliosis towards the affected side - in 79%, blurred or absent contour of the psoas muscle - in 78%, blurred shadow of the pyelocaliceal system on the excretory urogram - in 48%, a rarefaction halo symptom around the kidney - in 40%, deformation of the calyces and pelvis - in 38%, focal protrusion of the outer contour of the kidney shadow - in 9% of patients.
Excretory urography helps to identify the obstructive factor of the disease. On excretory urograms, in 68% of cases there is a sharp restriction of the movements of the kidney or its complete immobility when the patient breathes.
Forecast
in most patients A. n. bad, especially if you have a single kidney.
Treatment
. The patient is given intensive antibacterial therapy, prescribing broad-spectrum antibiotics, sulfonamides, nitrofurans. Treatment should be carried out taking into account antibiogram indicators. If ureteral obstruction is suspected, catheterization is necessary; Once the patency of the ureter is restored, a catheter is left in it for several hours.
With a low-virulent infection, the development of the purulent process in the kidney can stop and recovery occurs.
In cases where conservative treatment with antibiotics and chemotherapy, as well as catheterization of the ureter in order to restore the passage of urine through it, is not successful, and the patient’s condition continues to remain severe, surgical intervention is indicated.
The operation consists of exposing the kidney, its decapsulation, pyelostomy or nephrostomy. The largest pustules or their accumulations on the surface of the kidney should be opened, and the discovered carbuncles should be incised or excised. The operation is completed by applying cellophane-gauze swabs to the kidney. Removing a stone from the upper urinary tract, which is most often the cause of their occlusion, should be provided that this intervention is easily feasible within the existing surgical wound (pelvis, upper third of the ureter). If the stone is located lower and searching for it is difficult, then surgical intervention is limited to drainage of the kidney. Drainage from the kidney is removed only when patency of the urinary tract is completely restored. In the case of severe intoxication, extensive purulent damage to the kidney, the presence of multiple carbuncles in it, nephrectomy is indicated if the functional state of the second kidney is satisfactory (see Nephrectomy
).
Prevention
consists of timely treatment of extrarenal purulent foci, urological diseases, elimination of the causes leading to impaired outflow of urine from the upper urinary tract.
See also Kidneys
.
Bibliography
.: Panikratov K. D. and Gerusov Yu. M. Application of color thermography in the recognition of acute pyelonephritis, Urol. and nephrol., No. 4, p. 18, 1972; Pytel A. Ya. Pelvic-renal refluxes and their clinical significance, p. 199, M., 1959; Pytel A. Ya. and Goligorsky S. D. Selected chapters of nephrology and urology, part 2, p. 5, L., 1970; Fedorov S.P. Surgery of the kidneys and ureters, c. 3, p. 335, M.-Pg., 1923; Colby FH Pyelonephritis, Baltimore, 1959; Progress in pyelonephritis, ed. by E.H. Kass, Philadelphia, 1965; Pyelonephritis, hrsg. v. H. Losse u. M. Kienitz, Stuttgart, 1967.
A. Ya. Pytel
Sources:
- Big medical encyclopedia. Volume 2/Editor-in-Chief Academician B.V. Petrovsky; publishing house "Soviet Encyclopedia"; Moscow, 1975.- 608 p. with illustration, 8 l. on
Profiteroles to order with delivery - profiteroles delivery www.furshetnedorogo.ru.