Eye diseases › Heterophoria, eyes move differently
Heterophoria is asymmetrical and asynchronous eye movement, one of the forms of hidden strabismus.
Normally, the position of both eyes is balanced. This condition is called orthophoria. Healthy eyes work in sync and move in the same way. The position of the pupils, corneas and axes always coincides.
If one eye is deliberately closed, the second will move in sync with the first. The process of merging images obtained by both eyes into a single whole is possible only with orthophoria. Orthophoria occurs several times less frequently than heterophoria. With heterophoria, the eyes begin to work asynchronously. One eye closes and does not observe. The visual lines of the eyes diverge.
Classification
According to the direction of deviation there are:
- hyperphoria (top)
- hypophoria (down)
- excyclophoria, exophoria (outward)
- incyclophoria, esophoria (inside)
Visual acuity and performance depend on the angles of heterophoria. Manifestations of exophoria are compensated by the body up to 6 prismatic diopters, hyper/hypophoria - up to 1, esophoria - up to 3x.
Within these limits, the disturbances are not noticeable, although with constant visual work the eyes quickly get tired.
If the deviations exceed 8 diopters, the body is not able to combine the image from both eyes into a single whole. Decompensated heterophoria is formed. It is manifested by nausea, double vision, fatigue and poor health.
The disease progresses under stress, severe fatigue, overwork, and insomnia. Decompensated heterophoria can cause obvious strabismus. Pathological signs appear under conditions of stress, general weakening of the body, mental fatigue, and intense visual work. Decompensated heterophoria can lead to obvious strabismus.
Heterophoria – etiology and pathogenesis (causes and mechanism of occurrence)
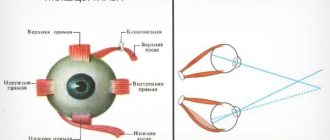
Etiology. Uneven force of action of the extraocular muscles.
Pathogenesis. Under normal conditions, thanks to the fusion ability of the visual analyzer, muscle imbalance does not manifest itself. When the eyes are separated (for example, by covering one eye or placing a prism on it with the base up or down), the relative weakness of any muscle begins to be revealed and the visual line of one of the eyes deviates inward (esophoria), outward (exophoria), upward (hyperphoria) ) or downwards (hypophoria), sometimes there is a deviation of the upper end of the vertical meridian of the cornea inwards (incyclophoria) or outwards (excyclophoria).
Diagnostics
Basic research methods for heterophoria:
- Maddox cylinder
- alternative cover test or cross-cover test
- fusion reserve test
The Maddox cylinder is used to study binocular vision and the condition of the retina in cases of cataracts. This is a red glass lens assembled from several surfaces in the shape of a cylinder. The surfaces are aligned along the same axis, the lens is included in the set of trial lenses.
The test determines the signs of strabismus and the state of muscle balance in both eyes of the patient. The patient puts on a frame with trial lenses. You need to monitor a light point 5 meters away.
A Maddox cylinder is placed in the frame of one eye. The patient can observe the light source with one eye as a point, and with the other as a strip - depending on how the axis of the cylinder is located. The coincidence of the dot and stripe indicates normal binocular vision. The discrepancy indicates strabismus, the degree of which will be determined by the magnitude (degree of angle) using prisms.
The idea of the cross-cover test is to limit binocular vision by observing the movement of the eyeballs. One eye is covered with a device, the lid of which is suddenly moved to the other eye. In persons with heterophoria, when moving the lid in the second eye, it is possible to see movement from the point of deviation.
Fusion reserves are examined with a synoptophore and variable prisms.
Reasons for development
Heterophoria can be provoked by the following factors on the human body:
- hereditary predisposition;
- congenital anomalies of the structure of the visual analyzer;
- lack of vitamins and minerals in the body;
- disruption of the innervation of the organ of vision;
- smoking;
- endocrine disorders;
- muscular paralysis;
- injuries;
- tumors;
- weakness of the muscles that move the eyeball;
- impaired immune defense;
- alcoholism;
- overwork;
- inactive lifestyle;
- frequent stress.
The accommodative ability of both visual organs may differ.
Heterophoria is an abnormality in the strength of the muscles between the right and left eyes. This process is facilitated by some anatomical features of the structure of the patient’s eyeballs. This is manifested in the difference in the position of the visual analyzers in the orbits, as well as the discrepancy between convergence and divergence. There may be differences in the severity of accommodation and opening of the palpebral fissure. Sometimes the tone of the circular muscles differs significantly.
Treatment
Heterophoria is treated with therapy or surgery. If the deviations do not exceed 3-4 prisms. diopter, vision can be corrected by changing the daily routine and creating the right conditions for work.
Basic means of vision correction:
- prescription of corrective lenses with decentering;
- eye gymnastics to restore fusion.
If the strength of the motor muscles in both eyes differs, wearing prismatic glasses is indicated. The base of the prisms is opposite to the deviation of the eyes. If the therapy is unsuccessful, the patient undergoes surgery to balance the eye muscles of both eyes.
HETEROPHORIA
HETEROPHORIA
(
heterophoria
; Greek beteros other, different + phoros bearing; syn.
hidden strabismus
) - deviation of the eyeballs from the correct (symmetrical) position with the exception of conditions for binocular vision.
The cause of G. is the unequal force of action of the extraocular muscles (muscle imbalance). In contrast to obvious strabismus, with G. binocular vision is always preserved (see).
G. occurs much more often (in 70-80% of people) than orthophoria (see). Under normal conditions, thanks to the fusion ability of the visual analyzer (see Fusion), muscle imbalance does not manifest itself. When conditions are created that exclude binocular vision (if one eye is covered), the relative weakness of a muscle is revealed, as a result of which the eye deviates towards the antagonist of this muscle. In this case, the visual line of this eye deviates inward (esophoria), outward (exophoria), upward (hyperphoria) or downward (hypophoria); sometimes there is a tendency to rotate the upper end of the vertical meridian of the cornea inward (incyclophoria) or outward (excyclophoria). Esophoria is more common than other types of vision. The degree of vision is determined by the deviation of the visual line of one of the eyes from the point of fixation and is expressed in prism diopters: 1Δ = 0.52°.
G.'s recognition usually does not present any difficulties. If you close one eye of the subject with your hand (the eye will deviate in one direction or another), and then open it, he makes an adjustment movement in the direction opposite to the one in which it was deviated. To determine the presence and nature of G., a prism or Meddox stick is placed on one eye (see Meddox stick, scale). Maddox's wand consists of a series of small red glass cylinders welded together. The light from the bulb is visible through it as a red line. The subject is asked to look at the light bulb by placing a Meddox stick to one eye. With G., the red line deviates in one direction or another from the light bulb. The direction of the image deviation will be indicated by the type of G., and the magnitude of the deviation on the tangential scale (a special cross with divisions corresponding to the tangents of the angles at a distance of the cross from the eye being examined is 1 and 5 d) or the strength of the prism, which transfers the image to the fixation point, is the degree of G.
With G., visual work, especially at close range, requires greater than usual neuromuscular tension to overcome the tendency of the eye to deviate. With high degrees of G. (7-8Δ and more) and weakened fusion ability, this can cause asthenopia (see), manifested by fatigue, headaches, nausea, transient diplopia (see). The occurrence of these phenomena is facilitated by general diseases, mental fatigue, and refractive errors.
When asthenopia occurs, it is necessary to create normal gigabytes. conditions for visual work, streamlining the daily routine; for ametropia and presbyopia - prescription of corrective glasses and orthoptic exercises (on a synoptophore or with the help of prisms) to restore fusion reserves. If there is no success, wear glasses with prisms directed at the apex in the direction of deviation of the eye, or (in exceptional cases) surgery on the external muscles of the eyes.
See also Strabismus.
Bibliography:
Avetisov E.S. Children's vision protection, M., 1975; Multi-volume guide to eye diseases, ed. V. N. Arkhangelsky, vol. 3, p. 274, M., 1962, bibliogr.; Sergievsky L. I. Concomitant strabismus and heterophoria, M., 1951, bibliogr.; Glaser T. Die Phorien, Ihre Prtifung und Korrektion, B., 1969; System of ophthalmology, ed. by S. Duke-Elder, v. 6, L., 1973.
E. S. Avetisov.
Prevention
To prevent the development of the condition, it is recommended to perform the following preventive actions:
- daily eye exercises, which should be carried out in the morning and evening; if a person works with a computer, it should be done every hour;
- good lighting in the room where a person constantly stays or works;
- annual examination by an ophthalmologist with all diagnostic procedures;
- examination of the baby by an ophthalmologist after birth and after some time.
Heterotrophy is often not detected in the early stages. This is due to the fact that the pathology is hidden. It is impossible to recognize it with the naked eye. That is why it is recommended to periodically visit an ophthalmologist immediately after the birth of children. He will be able to recognize the disease at an early stage and prescribe the necessary treatment.
Therapy for hidden strabismus
Up to 6 months, slight strabismus is considered a physiological norm; this is due to the fact that the eye muscles are still very weak. Over time, this phenomenon will correct itself. However, if persistent strabismus occurs as the child gets older, this is a reason to consult a specialist. Older children can talk about their problems themselves, but kids cannot understand what is happening to them.
If such alarming symptoms are present, parents should definitely take their child to the doctor.
The same methods are used for treatment in children. Of course, this is much more difficult, because it is very difficult to convince a child, for example, to constantly wear glasses or occlusion. At home, parents can themselves monitor whether the instructions are being followed correctly, but in kindergarten the child is often left to his own devices.
It is very convenient to use soft contact lenses for a child. Firstly, they are not visible on the face and the baby will not be teased. Secondly, the child will not be able to remove lenses, such as glasses. Of course, the lenses must be selected by the attending physician.
Surgical treatment of congenital strabismus is used before the age of 3 years. For acquired strabismus, surgery is indicated if there is no effect of therapy.
Therapy for hidden strabismus
A slight deviation of latent strabismus from the norm does not require specific therapy. In other cases, it is recommended to undergo examination and treatment.
To treat heterophoria, conservative treatment methods are used: glasses, the Synoptophore apparatus and visual gymnastics. Next, let's look at each of them in more detail.
For strabismus, it is very useful to perform gymnastics. The following exercises are suitable for this:
- straining your eyes, try to look at the tip of your nose for at least 7 seconds. Then comes relaxation with the eyes returning to their normal position for 3-4 minutes and everything repeats again;
- follow with both eyes an object that will be slowly moved by another person. In general, with strabismus it is very useful to observe moving objects;
- mentally drawing an infinity sign in front of your eyes or a figure eight - this greatly tightens your visual muscles;
- eye movements to the sides, in a circle;
- as you inhale, focus both eyes on the tip of your nose, and as you exhale, look into the distance;
- fast and strong repeated squinting gives a good load on the eye muscle;
- Try, if possible, to focus your gaze alternately on a close object, and then immediately on a distant one.
With hidden strabismus, the work of the extraocular muscles is impaired. The function of binocular vision forces them to remain in the correct position, but as soon as one eye is turned off from the visual process, the muscles of the other eye begin to work in a way that is more comfortable for them. In other words, hidden tension or weakness in certain extraocular muscles is compensated only when both eyes are working.
To detect hidden strabismus, it is enough to block the possibility of binocular vision, that is, close one eye. At the same time, it will deviate in the direction corresponding to the type of heterophoria. At the moment of restoration of binocularity, the pupil makes a characteristic adjustment movement and returns to the correct position. With orthophoria (absence of strabismus), the eyeballs remain in a consistent position under any conditions.
Due to constant overstrain of the oculomotor muscles in the process of synthesizing a binocular image, systematic headaches, a feeling of pressure and eye fatigue, nausea and dizziness may occur. To relieve such stress, it is recommended to constantly wear glasses with prismatic lenses. A prism with parameters of 2-3 degrees should be positioned with its base in the direction opposite to the direction of heterophoria.
If hypermetropia and myopia occur, sometimes corrective decentering glasses (changing the distance between the pupils upward or downward) are sufficient.
Synoptophore exercises give good results - training, relaxing and normalizing fusion reserves.
In some cases, hidden strabismus requires surgical intervention - the same as for obvious strabismus. However, the appropriateness of surgical assistance is determined by many factors (in particular, the degree of influence of the pathology on the patient’s quality of life).