Sensitive species
This group includes the olfactory, visual and auditory nerves.
The olfactory nerves have processes located in the nasal mucosa. Starting from the nasal cavity, they cross the cribriform plate and approach the olfactory bulb, where the first neuron ends and the central pathway begins.
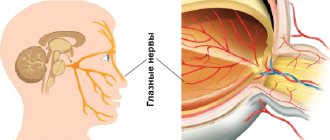
The visual pair consists of fibers extending from the retina, cones and rods. All nerves enter one trunk in the cranial cavity. First, they form a chiasm, and then the optic tract, which goes around the cerebral peduncle and sends fibers to the visual centers. One nerve contains about a million fibers (axons of retinal neurons) and, in addition, it has one sheath on the outside and another on the inside. The nerve enters the skull through the optic canal.
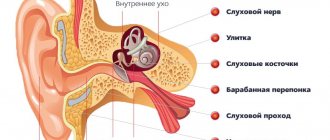
The eighth pair includes auditory cranial nerves - the remaining 12 pairs, except these three, are motor or mixed. In the auditory nerves, the fibers are directed from the middle ear to the nuclei. Each of them includes a vestibular and cochlear root. They arise from the middle ear and enter the cerebellopontine angle.
Research methods
The functional state of the vestibular-cochlear nerve is determined by a comprehensive study of the auditory and vestibular analyzers (see Audiometry, Vestibulometry). Vestibulometric, audiological and otoneurological research methods make it possible to differentiate P.'s lesions. n. within the inner ear or its root in the internal auditory canal and the cerebellopontine angle. When tonic diagnostics takes into account the possibility of involvement in the process of the V, VI, VII, IX, X cranial (cranial, T.) nerves, topographically combined with the vestibulocochlear nerve.
Motor types
Another group of 12 pairs of cranial nerves includes the oculomotor, trochlear, accessory, hypoglossal and abducens nerves.
The third pair, that is, the oculomotor nerves, contain autonomic, motor and parasympathetic fibers. They are divided into upper and lower branches. Moreover, only the upper branches belong to the motor group. They enter the muscle that lifts the eyelid.
The next group includes trochlear nerves that move the eyes. If you compare all the cranial nerves - 12 pairs - then these are the thinnest. They originate from the nucleus on the tegmentum of the midbrain, then go around the cerebral peduncle and go to the orbit, innervating the superior oblique muscle of the apple of the eye.
The abducens nerves are related to the rectus oculi muscle. They have a motor nucleus in the fossa. Coming from the brain, they go to the superior orbital fissure, innervating the rectus ocular muscle there.
Accessory nerves originate from the medulla oblongata and cervical areas of the spinal cord. The individual roots are connected into one trunk, passing through the hole and dividing into outer and inner branches. The internal branch, which contains fibers involved in the innervation of the larynx and pharynx, is attached to the vagus nerve.
And the last of the 12 pairs of cranial nerves (a table of which, for convenience, is presented at the end of the article), related to the motor ones, are the hypoglossal nerves. The origin of this nerve is spinal. But, over time, its root moved into the skull. It is clear that this is the motor nerve of the tongue. The roots emerge from the medulla oblongata, then cross the carotid artery and enter the lingual muscles, dividing into branches.
Mixed species
This group includes the trigeminal, facial, glossopharyngeal and vagus nerves. The mixed nerves have ganglia similar to those of the spinal nerves, but they do not have anterior and posterior roots. In them, the fibers of the motor and sensory types are connected into a common trunk. They can also just be nearby.
The output of the 12 pairs of cranial nerves is different. Thus, the third, seventh, ninth and tenth pairs have parasympathetic fibers at the output sites, which are directed to the autonomic ganglia. Many of them are united by branches where different fibers pass.
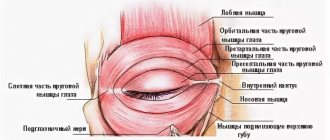
The trigeminal nerve has two roots, where the larger one is sensory and the smaller one is motor. Innervation of the skin occurs in the parietal, ear and chin areas. Innervation also includes the conjunctiva and apple of the eye, the dura mater of the brain, the mucous membrane of the mouth and nose, teeth and gums, as well as the main part of the tongue.
The trigeminal nerves exit between the cerebellar peduncle, in the middle, and the pons. The fibers of the sensory root belong to the ganglion, which lies in the temporal pyramid near the apex, which was formed as a result of splitting the dura mater of the brain. They end in the nucleus of this nerve, which is located in the fossa, as well as in the nucleus of the spinal tract, which continues into the medulla oblongata and then goes to the spinal cord. The fibers of the motor nerve root originate from the trigeminal nucleus, which is located in the pons.
The maxillary, mandibular and ophthalmic nerves depart from the ganglion. The latter is sensitive, divided into nasociliary, frontal and lacrimal. The innervation of the 12 pairs of cranial nerves varies not only among the pairs themselves, but also among their derivative branches. Thus, the lacrimal nerve innervates the lateral canthus, transmitting secretory branches to the lacrimal gland. The frontal nerve, accordingly, branches on the forehead and supplies its mucous membrane. The nasociliary nerve innervates the eyeball, and the ethmoidal nerves depart from it, innervating the nasal mucosa.
The maxillary nerve, which passes into the pterygopalatine fossa and exits onto the anterior facial surface, is also sensitive. The superior alveolar nerves originate from it and pass to the teeth of the upper jaw and gums. The nerve on the cheekbones passes from the ganglion along the posterior nerves of the nose to its mucosa and nasopharynx. The nerve fibers here are sympathetic and parasympathetic.
The mandibular nerve belongs to the mixed type. It consists of a motor root. Its sensory branches include the buccal nerve, which supplies the corresponding mucosa, the auriculotemporal nerve, which innervates the skin on the temples and ears, and the lingual nerve, which supplies the tip and back of the tongue. The inferior alveolar nerve is mixed. Passing in the lower jaw, it ends on the chin, branching here into the skin and mucous membrane of the lower lip. Its branches are connected to the autonomic ganglia:
- auriculotemporal nerve - with the ear, innervating the parotid gland;
- lingual nerve - with a ganglion that supplies innervation to the sublingual and submandibular glands.
The facial nerves include motor and sensory cranial nerves. Mixed fibers create a taste sensation. Some fibers here innervate the lacrimal and salivary glands, while others innervate the anterior two-thirds of the tongue.
The facial nerve consists of motor fibers that begin in the upper part of the fossa. It includes the intermediate nerve with taste and parasympathetic fibers. Some are processes of the ganglion, ending in taste fibers of the vagus and glossopharyngeal nerves. And others begin in the salivary and lacrimal nuclei, located next to the motor nucleus.
The facial nerve begins in the cerebellopontine angle of the brain and then enters the facial canal through the auditory canal. The chorda tympani is located here and, passing through the cavity, connects to the lingual nerve. It includes gustatory and parasympathetic fibers that reach the submandibular ganglion.
The facial nerve leaves the temple bone and passes into the parotid gland, intertwining there. From here the branches spread out in a fan-shaped manner. At this time, all muscles related to facial expressions and some others are innervated. A branch in the neck from the facial nerve branches on it in the saphenous muscle.
The glossopharyngeal pair supplies the innervation of the lacrimal glands, the posterior part of the tongue, the inner ear and the pharynx. Motor fibers are directed to the stylopharyngeal muscle and pharyngeal constrictors, and sensory fibers for the parotid gland are directed to the ear ganglion. The nuclei of these nerves, unlike where the other nuclei of the 12 pairs of cranial nerves are located, are located in the fossa - the triangle of the vagus nerve.
Parasympathetic fibers begin in the salivary nucleus. The glossopharyngeal nerve, leaving the medulla oblongata, reaches the base of the tongue. The tympanic nerve begins from the ganglion, which has parasympathetic fibers that continue to the ear ganglion. Next begin the lingual, tonsil and pharyngeal nerves. The lingual nerves innervate the root of the tongue.
The vagus pair provides parasympathetic innervation in the abdominal cavity, as well as in the chest and neck. This nerve includes motor and sensory fibers. This is where the greatest innervation is. The vagus nerve has a double nucleus:
- dorsal;
- single path.
Coming out behind the olive on the neck, it moves with the neurovascular bundle and then branches.
Spinal cord, medulla spinalis. Development of the spinal cord.
As already noted, phylogenetically the spinal cord (trunk brain of the lancelet)
appears at stage III of nervous system development (tubular nervous system).
At this time, there is no brain yet, so the trunk brain has centers for controlling all processes of the body, both vegetative and animal (visceral and somatic centers)
. According to the segmental structure of the body, the trunk brain has a segmental structure; it consists of interconnected neuromeres, within which the simplest reflex arc is closed. The metameric structure of the spinal cord is preserved in humans, which determines the presence of short reflex arcs in humans.
With the appearance of the brain (cephalization stage)
Higher control centers for the entire body arise in it, and the spinal cord falls into a subordinate position. The spinal cord does not remain only a segmental apparatus, but also becomes a conductor of impulses from the periphery to the brain and back, and bilateral connections with the brain develop in it. Thus, in the process of evolution of the spinal cord, two apparatuses are formed: the older segmental apparatus of the spinal cord’s own connections and the newer suprasegmental apparatus of the bilateral pathways to the brain. This structural principle is also observed in humans.
Decisive factor in the formation of the trunk brain
is adaptation to the environment through movement. Therefore, the structure of the spinal cord reflects the way the animal moves. So, for example, in reptiles that do not have limbs and move with the help of the body (for example, a snake), the spinal cord is developed evenly along its entire length and has no thickenings. In animals that use limbs, two thickenings occur, and if the forelimbs are more developed (for example, the wings of birds), then the anterior (cervical) thickening of the spinal cord predominates; if the hind limbs are more developed (for example, the legs of an ostrich), then the posterior (lumbar) thickening is increased; if both forelimbs and hindlimbs (four-legged mammals) are involved in walking, then both thickenings are equally developed. In humans, due to the more complex activity of the hand as a labor organ, the cervical thickening of the spinal cord was differentiated more strongly than the lumbar one.
The noted phylogenetic factors play a role in the development of the spinal cord and ontogenesis
.
The spinal cord develops from the neural tube,
from its posterior segment (the brain arises from the anterior segment). From the ventral section of the tube, the anterior columns of the gray matter of the spinal cord (cell bodies of motor neurons), adjacent bundles of nerve fibers and processes of these neurons (motor roots) are formed. From the dorsal section arise the posterior columns of gray matter (cell bodies of interneurons), posterior funiculi (processes of sensory neurons).
Thus, the ventral part of the brain tube is primarily motor
, and the dorsal one is
primarily sensitive
.
The division into motor (motor)
and
sensory (sensitive)
areas extends throughout the neural tube and is maintained in the brain stem.
Due to the reduction of the caudal part of the spinal cord, a thin cord of nervous tissue is obtained, the future filum terminale.
Initially, in the 3rd month of uterine life, the spinal cord occupies the entire spinal canal, then the spine begins to grow faster than the brain, as a result of which the end of the latter gradually moves upward (cranially). At birth, the end of the spinal cord is already at the level of the third lumbar vertebra, and in an adult it reaches the height of the first - second lumbar vertebra. Thanks to this “ascent” of the spinal cord, the nerve roots extending from it take an oblique direction.
Violations
All cranial nerves—12 pairs—may have dysfunction. The anatomy of the lesion sites appears at different levels of the nuclei or trunks. To make a diagnosis, an in-depth analysis of intracranial pathological processes is performed. If the lesion affects one side of the nuclei and fibers, then most likely we are talking about dysfunction of any of the affected 12 pairs of cranial nerves.
Neurology, however, also studies symptoms on the opposite side. Then damage to the pathways is diagnosed. It also happens that dysfunction of the nerves is associated with a tumor, arachnoid cyst, abscess, vascular malformations and other similar processes.
Simultaneous damage to the 12th pair of cranial nerves, that is, the hypoglossal, as well as the vagus and glossopharyngeal, is called bulbar palsy. This is a very dangerous disease, since there is a possibility of pathology of the most important centers of the brain stem.
Knowledge of the topographic location of the cranial nerves allows one to correctly identify the narrow area of damage to each of them. To conduct research, special techniques are used. With the appropriate equipment, today it is possible to identify all the details of the condition of the fundus, optic nerve, diagnose the visual field and areas of loss. Computerized examination allows highly accurate localization of the affected area.
Treatment of the disease
Treatment of nasociliary nerve neurosis consists of eliminating the disease that affects it.
In case of inflammatory processes in the ENT organs, patients are prescribed a course of treatment with antibiotics and a set of drugs that affect the elimination of inflammation and restoration of the mucous membrane, or surgical intervention (for pathologies of the nasal septum).
For vascular diseases, patients are prescribed drugs with antihypertensive and nootropic effects. Treatment is also carried out using vasoactive drugs.
To relieve pain and other symptomatic and clinical manifestations of neuralgia, local anesthetic drugs are used in medical practice in combination with non-narcotic painkillers and vasodilators. Their use is determined by which part of the nasociliary nerve has undergone pathological effects:
- For neuralgia of the long ciliary nerve, dicaine (0.25% eye solution) mixed with adrenaline (4 drops per 10 ml of solution) is used.
- For neuralgia of the subtrochlear region of the nasociliary nerve, cocaine hydrochloride (2% solution) mixed with 0.1% adrenaline (4 drops per 5 ml of the drug) is used. A solution of lidocaine is also used in the form of a spray, which is injected into the nasal passages on the corresponding side or both at once (for bilateral neuralgia) up to 4 times a day.
- If any part of the nerve is damaged, use a powder mixture of papaverine, glucose, antispasmodic, diphenhydramine and aminazine 2 times a day.
As an additional therapy for patients diagnosed with Charlin's syndrome, a course of intramuscular vitamin B12 is indicated, as well as intravenous administration of sulfonamide drugs.
Unpleasant chest pain is often a sign of heart disease. But a similar symptom is also characteristic of neuralgia. A competent specialist should be able to distinguish the signs of neuralgia in the heart area from heart pain. Read the article about how to treat this disease.
We will consider the causes and symptoms of trigeminal neuralgia in this topic.
Neurological examination and symptoms of disorders of individual cranial nerves
This technique is carried out in a certain order. The examination begins with the olfactory nerve. A cotton wool soaked in the irritant is brought to the nostrils one by one. The optic nerve is examined during an ophthalmological examination, based on which, in addition to direct damage, it is possible to identify even secondary changes. The pathology can be stagnant, dystrophic, inflammatory, or the nerve can be completely destroyed.
Lesions of the following three of the 12 pairs of cranial nerves (oculomotor, abducens and trochlear) cause diplopia and strabismus. Drooping of the upper eyelid, dilation of the pupil, and double vision may also occur.
Disturbances in the fifth pair, that is, in the trigeminal nerves, lead to a deterioration in sensitivity in the part of the face where they are present. This can be observed in the area of the temples, forehead, cheekbones, eyes, chin and lips. It happens that severe pain is felt, rashes and other reactions appear. Due to the fact that the facial nerves have many connections, this pair is characterized by a wide variety of pathological reactions.
If the auditory nerve is damaged, hearing deteriorates; the glossopharyngeal nerve impairs sensitivity in the inner ear; the sublingual nerve causes limited movement of the tongue. In the case of the vagus nerve, paralysis of the soft palate or vocal cord develops. In addition, the rhythm of the heart, breathing, and other visceral-vegetative functions may be disrupted.
Diagnosis of neuralgia
A neurologist is involved in differential diagnosis. Diagnosis of neuralgia begins with a neurological examination of a patient with typical complaints for this disease. The listed causes of neuralgia require a more complete examination to identify or exclude the underlying disease.
In some cases, additional instrumental examination (electroneurography) may be required if the cause of neuralgia was injury in the projection of the nerve. An MRI of the spine or any of the nerve plexuses may be required in the event of any volumetric impact on the nerve structures, as occurs with a herniated or protruded intervertebral disc or soft tissue tumors.
Complex disorders and cranial nerves (12 pairs): anatomy, table
The functions of nerve fibers can be impaired either isolated or in combination, together with various pathologies of the lower skull. So, if all the nerves on one half of the cranial base are affected, then they talk about Garcin syndrome. When there is a tumor of the orbital bones and soft tissues, superior orbital fissure syndrome occurs. When both the hug and optic nerves are damaged, Kennedy syndrome occurs.
These and other diseases occur in both adulthood and childhood. For children, nerve damage that is associated with developmental defects is especially common.
Below is a structure that can help you better understand how the cranial nerves (12 pairs) work. Anatomy (the table is based on her knowledge) will help you navigate the intricacies of the functioning of their different groups.
Diagnostics
Diagnosis is based on symptoms, medical history, and research:
- The doctor talks with the patient, finds out the symptoms. Finds out what the pain is and where it is located. Are there any infectious diseases in the head area? For example, otitis media, sinusitis, tooth extraction, adenoiditis.
- Then he examines and palpates the damaged area. The presence of swelling and redness is detected.
- When the doctor roughly presents the diagnosis, he examines for the presence of diseases with similar symptoms. That is, differential diagnosis is carried out. Refers for examination to a dentist and otolaryngologist.
- To determine the diagnosis, there is a method of applying a solution of cocaine hydroxide to the mucous membrane of the front of the nose. If the patient stops feeling pain, then this is inflammation of the nasociliary nerve.
- Next, instrumental studies should be carried out. Ophthalmoscopy, MRI of the head, biomicroscopy, anterior rhinoscopy.
- Once the diagnosis is made, treatment is prescribed.
With the help of additional examination, neuralgia of the nasociliary nerve is differentiated from other diseases. And they establish an accurate diagnosis.
Biomicroscopy of the eye
This is done using a slit lamp, the main part of which looks like a large slit. The device examines the structure of the eye, the back and front walls. This method allows you to see any damage, foreign body, and detect the disease at an early stage. Biomicroscopy allows you to see the condition of the retina and optic nerve.
Ophthalmoscopy
The fundus of the eye is examined using an ophthalmoscope. With the help of an eye mirror you can see blood vessels and nerves. Identify changes, redness, swelling.
Anterior rhinoscopy
This is done using a nasal speculum.
The anterior part of the nasal cavity is examined by inserting the device into the nostrils. The most suitable for this procedure is the Hartmann mirror. The doctor holds the device in his left hand, slightly dilating the nostril. In this case, the nasal septum and passages are visible. This is how redness, curvature, atrophy and hypertrophy are noticed. Sometimes it is possible to examine the nasal cavity using reflector lighting. It is used to examine children, as they may be frightened by an unknown object.
MRI of the head
To accurately confirm the diagnosis, an MRI of the head is performed. X-ray radiation is not used here. The examination is carried out using magnetic fields, which create an energy change in the examination area. This is how photographs are taken without the use of contrast. A cross-sectional image is displayed on the computer monitor.