Skiascopy: what is the essence of the method?
Our eyes are a system that perceives electromagnetic radiation and provides visual function. It has a complex structure and processes a large amount of information in seconds. In the absence of diseases, the visual system fulfills its purpose, creating the correct sensation of the position of objects in space. In the presence of negative factors, ophthalmological diseases occur, which are manifested by decreased vision. People also develop myopia, acquired astigmatism, and hypermetropia.
Regular visits to doctors is an effective method by which you can avoid the above problems. To diagnose the functional functioning of the eyes, ophthalmologists use a proven method called skiascopy. It has been used for many years and is trustworthy. It is used to determine the ability of the visual organ to refract light rays.
Skiascopy is an objective method that is based on observation of a moving shadow. The first research was carried out in 1873. The technology was introduced by the famous French scientist Cunier. He developed an effective technique that is still used today. This suggests that during the procedure, specialists obtain the correct results.
Skiascopy, what is needed for the procedure?
There is no need to take any specific tests before starting the procedure. All you need for diagnostics is a fairly dark room, a light source (an ordinary electric lamp works well for this function), and a skiascope - a special device with additional rulers in the set.
What is a skiascope and skiascope rulers?
- The skiascope appears in the form of an unusual mirror. One side of it is straight, and the other is in the shape of a concave lens. In the center of this mirror there is a hole through which the specialist will observe the shadows formed in the visual organ. This kind of mirror is attached to the handle.
- The set of skiascopic rulers consists of two pieces. Each such ruler is represented as a frame with ten lenses. Each subsequent lens differs from the previous one by 1 diopter - a unit of measurement of visual acuity. To ensure accurate results, the ruler design has an additional attachment. It reduces each ruler step by 0.5 diopters. One of these rulers has magnifying lenses, and the other has the opposite meaning.
Important: From information sources you can find out that skiascopy is possible using ordinary lenses that are designed for selecting glasses, as well as an ophthalmoscope. This is true, but the specialist conducting such diagnostics must have extensive experience and have certain skills.
Diagnosis of astigmatism is carried out using a set of cylindrical lenses - they differ in the presence of an axis.
FEATURES OF SKIASCOPY
Examination of the pupils or skiascopy is carried out using a special device called a skiascope. It has the shape of a round mirror with a handle. One part of the mirror is concave inward, and the second is flat. In the central part, the skiascope has a hole through which the eye is examined.
Skiascopy is carried out by directing a stream of light into the patient’s pupil, while the doctor controls the reaction of the light spot. This spot forms on the fundus of the eye. When the skiascope is rotated, the shadow may move, indicating refractive errors.
Skiascopic examination allows us to identify the degree of refractive error with maximum accuracy. This technique is appropriate in the following cases:
- allows you to study refraction in children if they cannot talk about symptoms;
- identify false information when a patient is faking during an eye exam;
- determine refraction in people with intellectual disabilities.
The essence of skiascopy
A skiascope is an instrument that is a round mirror with a handle. One side is concave and the other is flat. The center of the skiascope is equipped with a hole through which the doctor observes the eye of the subject.
Using this instrument, the ophthalmologist directs a beam of light into the patient’s pupil and observes the reflex - a light spot that forms on the fundus of the eye. When the skiascope is rotated, the shadow moves and reports certain changes in refraction.
Skiascopy makes it possible to accurately determine the degree of refractive error . This is especially important in the following cases:
- The patient deliberately feigns illness;
- Examination of young children who cannot talk about their complaints;
- Patients with intellectual disabilities.
Existing contraindications
There are no serious contraindications to the skiascopy procedure. It is not recommended to use this method for patients with serious psychological illnesses (especially if they are in the acute stage), as well as for people with photophobia.
Before the procedure, the patient is instilled with special drops that help the ciliary muscle relax and not react so sharply to exposure to light. It is this feature of the procedure that can create difficulties in diagnosis. For some people, the use of such drugs is contraindicated and skiascopy must be performed without their use. This may affect the reliability of the results.
Important: Many patients over 35 years of age may begin to develop a latent form of glaucoma. This method can provoke its sharp development. To avoid this, before starting the procedure, patients over this age must have their intraocular pressure measured.
Carrying out skiascopy
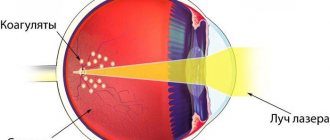
The whole essence of the method is to reflect directed light onto the retina of the eye organ. If the patient has impaired refraction, the reflected shadow will be shifted. It is impossible to stimulate such an effect on your own. That is why skiascopy is one of the most reliable methods for diagnosing refraction.
As mentioned earlier, before the procedure begins, the patient’s eyes are instilled with special cycloplegic compounds. Most often, these drugs are Atropine or Cyclomed, but they have certain contraindications for use. Therefore, if a person has health problems such as diabetes, hypertension, glaucoma, or an allergic reaction to drug components, an ophthalmologist should be informed about this.
When the medicine begins to work, the specialist takes the patient into a dark room and sits him on a chair. A light source is installed behind. The doctor himself moves away from the patient by 0.67 or 1 meter.
Using a skiascope, a specialist directs a beam of light directly into the pupil of the eye organ and begins to observe the shadow that is formed from the reflected light. To do this, the skiascope is first slowly turned vertically, and then horizontally.
Throughout the procedure, the specialist asks the patient to look at the center of the mirror, namely at its hole. But this rule applies to those patients who have undergone preliminary instillation and their accommodation is relaxed. If the procedure is carried out without the use of special means, the patient will need to look past the specialist’s ear.
Next, the specialist observes the point of reflected light. Her movements will depend on the side of the mirror. If the mirror was turned to the straight side, the point moves in the same direction as the mirror, but this is only in the case when the patient’s vision is normal or there is mild myopia. With farsightedness, the point of light moves in the direction opposite to the mirror. If the mirror was used with the side of the concave lens, all the above movements of the point of light will be opposite.
Features of skiascopy
The author of the method for studying the refractive power of the eye is considered to be the French physician Cunier, who first used it in 1873.
The term skiascopy is derived from the Greek words skia and skopio - shadow and looking. You can also find the name of the procedure retinoscopy (retina - retina). The procedure is carried out in a dark room using:
- light source (frosted light bulb with a power of 60-80W);
- a skiascope device, consisting of two mirrors - flat and concave;
- skiascopic rulers with a set of lenses.
The light bulb is placed behind the patient's head, on the left side. Using a flat mirror of a skiascope, the doctor directs a beam of light rays reflected from the lamp into the eye of the person being examined. A spot of light appears in the pupil area. If the mirror is rotated in different directions around the vertical and horizontal axes, shadows will appear. Based on the direction of movement of the shadow, the type of refractive error is determined (myopia, farsightedness, astigmatism), and with the help of skiascope ruler lenses, the magnitude of the refraction is determined.
Interpretation of the skiascopy results, like the procedure itself, should be carried out by an experienced doctor. In this case, the degree of visual impairment can be determined with high accuracy. If the doctor does not have enough experience, the results may be distorted.
Skiascopy is similar to refractometry. These two studies are interchangeable. But, unlike refractometry, skiascopy does not require special equipment, but is carried out manually by a doctor.
HOW THE RESEARCH IS CONDUCTED
The skiascopy technique is carried out in a special dark room. In order to carry out skiascopic manipulations, the following tools are required:
- Skiascope.
- A set of rulers for skiascopes, which are equipped with negative and positive lenses.
- Electric incandescent lamp.
Before making a diagnosis, the doctor instills special medications into the patient’s eyes to dilate the pupils. This is done in order to obtain the most accurate results. After this, the doctor sits the patient on a regular chair and begins the examination:
- at eye level on the left side there is a switched-on electric lamp;
- using a skiascope, a light beam is directed into the patient’s eye;
- the beam reaches the fundus of the eye, after which the doctor begins to rotate the mirror in different directions.
At this moment, movement of the shadow is observed, from which conclusions are drawn about the refraction of the eyes.
It is important to know! To carry out such diagnostics, it is not necessary to use a skiascope. Instead, a retinoscope can be used, and the rulers are replaced with ordinary lenses.
Skiascopy does not necessarily require pupil dilation. When performing skiascopy, the doctor may ask the patient to simply look behind his ear.
Preparation for the procedure and sequence of procedures
Skiascopy: a device
The refractometry method does not require special preparation. It is offered by many public and private ophthalmology clinics throughout the country.
There are some contraindications to the use of the technique. Refractometry is not prescribed to patients with mental illness and persons under the influence of drugs or alcohol.
To increase the accuracy of the study, it is possible to use medications by instilling them into the patient’s eyes in order to reduce the blinking function, although most often this is not necessary, since the procedure lasts a very short time.
At the appointment, the ophthalmologist, at the request of the patient, can tell about the method called “skiascopy” and what it is. During the measurement process, the patient assumes a sitting position. The doctor is located at a distance of one meter, 50 or 67 centimeters from him and turns on the skiascope - a flat or concave mirror with a source of narrowly focused lighting.
During the procedure, the mirror is rotated along the horizontal and vertical axes in different directions and the nature of the movement of the shadow formed from the light beam along the fundus of the eye is observed, which, when the beam hits it, is highlighted in red.
The following video will introduce you to the procedure:
WHO IS THE PROCEDURE FOR?
Skiascopy is an eye examination procedure, so it is intended for those people who have vision problems. Skiascopy is indicated for the following ophthalmological diseases:
- farsightedness;
- myopia;
- astigmatism.
Skiascopy is also indicated in cases where it is necessary to determine the effectiveness of treatment, as well as to determine the rate of progression of eye diseases. This method has many advantages, but despite this, there are also a number of contraindications.
CONTRAINDICATIONS TO THE STUDY
Shadow eye refraction is contraindicated for persons with the following diseases and pathologies:
- Fear of light, through which the patient experiences increased sensitivity to light flux.
- Skiascopy can be performed on children no earlier than 7 years of age.
- If the patient is under the influence of alcohol or drugs.
- If you have glaucoma or suspect it.
- In the presence of acute chronic diseases, through which it is possible that the patient may “break loose” and cause harm to himself or others.
Who should not undergo skiascopy?
Despite the simplicity and harmlessness of the method, skiascopy has a number of contraindications :
- Photophobia (increased sensitivity to light);
- Glaucoma or suspicion of it (the study may cause an acute attack of this disease);
- Skiascopy in children is contraindicated under 7 years of age;
- State of alcohol or drug intoxication;
- Acute mental illnesses in which patients can cause harm to themselves and others.
Skiascopy: step-by-step process
The human eyes are an optical system that is capable of light refraction. Visual function is provided by the lens and cornea. Skiascopy is ideal for determining eye refraction. With its help, you can easily identify disorders that are difficult to determine through viziometry.
The word "skiascopy" consists of two parts. Translated from Greek, it means “shadow” and “I watch.” This is an instrumental diagnostic method carried out in several stages:
- First, a special short-acting agent is instilled into the eyes. The most commonly used is Cyclodol. This is a medication that causes paralysis of the ciliary muscle of the eye. Atropine is also used. It is an alkaloid found in plants of the nightshade family. It causes cycloplegia
- at the next stage, the person enters a darkened room and sits on a chair. Opposite him, at a distance of more than half a meter, is a doctor. It directs a beam of light emanating from a lighting device into the eyes of the person being examined.
- the ophthalmologist picks up a skiascope. This is a tool with a simple design. It is a small mirror with a concave and flat side. There is a hole in the center of the skiascope. Through it, the ophthalmologist monitors the patient's eyes
- Using a two-way mirror, the doctor directs a beam of light into the pupil and closely observes the reflexes. He slowly rotates the tool around an axis and draws conclusions based on the nature of the movement of the shadow
- Skiascopic rulers are used when conducting the study. For example, from the Japanese manufacturer Inami. The kit includes positive and negative lenses. A person applies simple devices to his eyes, and the doctor watches when the shadows stop moving. The size of the lens needed to neutralize shadows is a significant indicator. It determines the degree of refraction of the eyes
Skiascopy is a technique that opens up wide opportunities for ophthalmologists. With its help, you can identify disorders of the visual system and successfully correct them. After receiving the results, the doctor prescribes glasses or contacts. These are optical devices designed for vision correction. They are used to correct refractive errors.
Depending on the type of lenses used in the study, there are several methods for determining refraction. For example, to determine the degree of astigmatism, cylindroskiascopy is performed. A trial spectacle frame is placed over the eyes. The socket accommodates spherical and astigmatic lenses. They provide simultaneous neutralization of shadows. First, the ophthalmologist turns the mirror with the hole towards the astigmatic lens. If the shadow disappears, neutralization of ametropia is achieved. Ametropia means a change in the refractive power of the visual organ. After this, the specialist carries out other actions aimed at determining the level of refraction. At the end of the procedure, the doctor gives an opinion and provides qualified recommendations.
Bar-skiascopy is considered a separate type of research. This is a process carried out using special devices. Their key difference is the formation of a light source in the form of a strip. To assess refraction, the ophthalmologist determines the direction of movement of the shadow. Strip skiascopy is widely used to determine refraction in schoolchildren. It is characterized by high accuracy and reliability.
When performing skiascopy and making a diagnosis, the medical professional pays attention to the following important points:
- rulers with lenses should be held strictly vertically and placed at a distance of 12 mm from the top of the convex part of the eyeball. Then the results obtained will be as accurate as possible
- after using Cyclodol or Atropine, the patient looks at the hole in the mirror. If accommodation (adaptation of the eye to changes in external conditions) is preserved, the patient should look past the doctor's ear
- the absence of a shadow on the pupil of the eye when conducting a study from a distance of one meter indicates that the person has myopia - 1.0 diopters
- interpretation of the results depends on which mirror is used (flat or concave)
- the unstable nature of the movement of the shadow indicates insufficiency of cycloplegia, as well as the negative impact of accommodation on the final results
- The shadow test is carried out in a darkened room. An electric lamp is placed on the table. During the procedure it turns on
How is skiascopy performed?
The study is carried out in a dark room . It should contain the following equipment:
- Skiascope;
- Electric lamp;
- A set of skiascopic rulers: one with negative lenses, the other with positive ones.
Sometimes, instead of a skiascope, a retinoscope is used, and instead of skiascope rulers, ordinary lenses are used, which are used when selecting glasses.
Before the study, the patient undergoes cycloplegia - dilation of the pupil by instilling cyclodol or atropine. Such an event increases the accuracy of the result.
The patient sits on a chair at a distance of 0.67 to 1 m from the doctor. On the left side, at eye level of the subject, there is a switched-on lamp. Using a skiascope, the doctor directs a light beam into the patient's eye, which falls on the fundus of the eye, and then turns the mirror in different directions. At the same time, the shadow moves and allows us to judge the refraction of the eye.
If cycloplegia was performed, the patient looks at the opening of the skiascope during the examination. If the pupil is not dilated, you need to look behind the doctor’s ear.