PET/CT examination - what is it?
The deciphering of the abbreviation sounds like positron emission tomography - computed tomography. This diagnostic method combines the study of the structure and functional characteristics of tissues. The technology is especially widely used in oncology to identify and determine the degree of development of malignant tumors.
Why?
Today, up to 90% of PET/CT studies in the world are performed on people suffering from cancer. The study is important from a number of perspectives:
- The study is important from the point of view of determining the degree of development and spread of the tumor process, detection of metastases, both regional and distant.
- In medical practice, there are situations when doctors are unclear about the nature of the process occurring in a particular organ. The study allows you to differentiate the process, distinguish between benign and malignant.
- The study helps to understand whether the treatment is effective.
- The study can be used to diagnose relapse of the disease.
When it comes to diagnosis, many cancers have the ability to actively accumulate fluorodeoxyglucose. This substance is used during the study. However, some types of cancers have low metabolism.
These types include:
- Highly differentiated cancerous neoplasms of the thyroid gland; Benign tumors of any location;
- Some kidney tumors;
- Some bone tumors;
- Liver tumors;
- Prostate tumors;
- Some types of sarcomas, lymphomas.
Having a low metabolic rate, they are poorly visualized by PET/CT. This means that other diagnostic methods are required.
PET center of the Federal State Budgetary Institution "National Medical Research Center for Cardiovascular Surgery named after. A.N. Bakulev" of the Ministry of Health of Russia
What is PET?
PET (positron emission tomography) is a modern, highly sensitive nuclear diagnostic method that allows you to evaluate various metabolic processes occurring in organs and tissues. The method is based on the ability to monitor the distribution in the body of biologically active compounds labeled with positron-emitting radioisotopes.
PET/CT (positron emission tomography combined with computed tomography) - allows you to study physiological and pathophysiological processes in one study, as well as compare them with the anatomical and topographical features of the structure of organs and tissues.
This is possible due to the fact that the method consists of two modalities:
- PET (positron emission tomography) – functional assessment;
- CT (computed tomography) – anatomical and structural assessment.
to diagnose the entire body in one study : from the level of the eye sockets to the upper third of the thigh (if necessary, the examination area is expanded).
Cost of PET/CT and PET studies
PET/CT of the whole body with 18F-FDG – 51,000 rubles.
ATTENTION!
In the PET center of the National Medical Research Center for Cardiovascular Surgery named after. A.N. Bakulev it is possible to perform PET/CT examination FREE OF CHARGE for the patient:
- compulsory medical insurance (payment from the compulsory health insurance fund). Read more >>>
- by bank transfer at the expense of insurance companies - details when registering for the study and by phone. Economic Department of the National Medical Research Center for Agriculture named after. A.N.Bakuleva +7 (495) 414–75–67.
Nonresident patients can use the hotel services on the territory of the National Medical Research Center for Cardiovascular Surgery named after. A.N. Bakuleva - details by phone. +7 (495) 414–75–46.
Registration for the study
ATTENTION!
All PET examinations are carried out by appointment. Registration for studies is carried out daily, except Saturday and Sunday, from 13:00 to 17:00 only by phone
ATTENTION:
It is necessary to follow certain rules of preparation before the study.
- Reminder for a patient scheduled for a PET/CT or whole body PET study with 18F-FDG
- Reminder for the patient booked for PET/CT of the whole body with 11C-choline
- Reminder for a patient booked for a PET scan of the brain with 11C-methionine
- Memo for a patient scheduled for 13N-ammonium myocardial PET/CT
Driving directions
Address:
121552, Moscow, Rublevskoe shosse, 135. Federal State Budgetary Institution "NMITs SSH im. A.N. Bakulev" of the Russian Ministry of Health. The center is located at the intersection of Rublevskoye Highway and the Moscow Ring Road.
Travel by public transport:
- From Art. metro station "Molodezhnaya". Exit from the first carriage. Bus No. 660 and minibus No. 660, to the stop “Center for Cardiovascular Surgery named after. Bakulev". Stop opposite the checkpoint.
- From Art. metro station "Krylatskoe". Exit from the last car, to the right. Buses No. 129 and 376, minibuses No. 358 and 376, go to the Cherepkovo stop, cross the underground passage to the opposite side and go up the path to the Center. Prohodnaya, closest to Rublevskoye Highway. A separate entrance under the canopy (on the right, closest to the entrance) with a sign “PET center”.
The receptionist will meet you and take you to the doctor.
Description of research technology
The basis of the research technology is the study of tissue characteristics, structural and functional. Functional characteristics can be assessed through metabolism. Let's take the following example. We choose a substance that is necessary for all cells of the body. We mark it with a radioactive label, introduce it into the body and observe the places of its maximum accumulation.
Glucose is a universal substance in the human body. With the help of glucose, almost all tissues and cells are nourished. In malignant tumors, the greatest consumption occurs, since the growth and reproduction of tumor cells requires a lot of energy.
In a PET/CT scan, glucose is labeled with radioactive atoms with a short half-life. Once in the body, glucose actively accumulates in tissues with the most intense metabolism, i.e. in cancerous tumors.
The tag disintegrates, emitting energy in the form of gamma rays. A special device records this process. The data that the doctor receives creates a visual model showing the location of the tumor, its size and metastases.
Radioactive tracers accumulate only at the location of atypical cells; healthy tissues are not visualized.
When the doctor needs to examine both healthy and changed structures, CT comes to the rescue, allowing you to obtain a detailed picture with millimeter accuracy.
After data from both scanning systems is received, they are superimposed on each other, thereby achieving an image that gives a clear picture of the location of tumor foci.
Combining different visualization methods
Diagnostic capabilities are expanding not only through the use of new radiopharmaceuticals that are more sensitive to changes in metabolism in certain areas. Visualization technologies are also being improved by combining them.
The first devices for examination using the positron emission tomography method showed areas with pathological processes, but did not provide sufficiently accurate information about their location in the tissues. To obtain a more accurate clinical picture, PET and CT studies were combined.
PET with CT
Installations that combine positron emission tomography and computed tomography have become standard today and have significantly improved the information content of scanning results. For example, if a PET study of a lesion is carried out as part of preparing a patient for stereotactic radiosurgery, the information content of positron emission tomography is not always sufficient to determine the exact anatomical boundaries of the tumor, and, therefore, guarantee the safety and effectiveness of treatment.
In this case, a comprehensive examination is indicated: PET in combination with CT. For these purposes, special hardware systems are used that allow both types of diagnostics to be carried out simultaneously. Using CT, the anatomy of the pathological focus is determined, and a positron emission tomograph provides information about the metabolic activity of tissues in problem areas.
Thus, the diagnosis of PET in combination with CT allows the doctor to obtain information that neither of these studies performed separately can provide.
Today, based on the results of PET CT examination:
- diagnostics are carried out to identify areas with pathologies if cancer is suspected;
- not only the presence of large tumors is determined, but also the presence of metastases;
- the effectiveness of treatment is assessed and its further tactics are determined;
- the question of the possibility and nature of surgical intervention is resolved;
- the procedure for radiosurgical treatment and other types of radiation therapy is determined;
- The condition is monitored after treatment, and relapses of the disease are detected.
PET with MRI
Currently, developments are actively underway and the first samples of installations combining PET with MRI have appeared. For a number of cases, the use of MRI will be more informative than the use of computed tomography. Magnetic resonance imaging allows you to get an accurate image of all tissues, and it is not obscured by bone structures, as is the case with CT. An additional advantage of using MRI combined with positron emission tomography will be a reduction in radiation exposure to the patient’s body. MRI is not a radiological examination method. The first examples of PET MRI units appeared in Israel and the USA. In Russia, unfortunately, at the moment there is no such equipment yet.
Types of drugs used
The potential of a study depends on the arsenal of radiopharmaceuticals used in it. These drugs are labeled with unstable isotopes that make them radioactive.
Today, isotopes of such elements as:
- Nitrogen-13;
- Oxygen-15;
- Carbon-11;
- Fluorine-18.
In oncology, fluorine is most common, since it has the longest half-life and at the same time the lowest radiation energy.
These advantages of fluorine make it possible to obtain high-quality images with high spatial resolution. In addition, the relatively long half-life makes it possible to transport the drug from the site of production to the clinic.
The most common drug used is fluorodeoxyglucose. It is an analogue of glucose. Atypical cells absorb it faster, it actively accumulates, and this is ideal for scanning.
The downside of fluorodeoxyglucose is that it accumulates in brain tissue and nephrons, which in turn can cause these organs to glow, even when they are healthy.
This drawback stimulated the search for other, more advanced drugs, and now such drugs have been created.
An example of a modern drug is 18F-FET. It is intended for the brain and contains the amino acid tyrosine, labeled with the fluorine-18 isotope. Tyrosine has a very high selective accumulation in brain tissue, which is important for imaging neurotumors.
The drug is also used to diagnose oropharyngeal tumors, to detect metastases and to diagnose lesions of the cervical lymph nodes.
What is PET CT
Positron emission tomography (PET) is one of the most informative methods in the early diagnosis of serious diseases: cardiac, neurological, including oncological.
The essence of the method
During the study, using a PET scanner, pathological changes are recorded at the molecular level, due to which diseases are detected already at the initial stage, before symptoms appear. The high diagnostic accuracy of the PET CT method is achieved through a combination of two imaging technologies: positron emission tomography and computed tomography. PET allows you to obtain data on the functional characteristics of the body, and CT makes it possible to correlate images of sections of the studied area with anatomical characteristics and recreate a three-dimensional model of the organ.
PET CT image interpretation shows:
- localization, structure, size of the pathological focus;
- degree of aggressiveness of cancer cells;
- stage of development of the neoplasm;
- organs affected by metastases;
- results of previous treatment.
PET examination is classified as a nuclear medicine method. Radiopharmaceuticals are used to detect pathological processes. Isotopes enter the patient’s body in safe minimal doses. The dosage in each case is calculated individually. Radioactive tracers are administered intravenously by injection or through the lungs using a special inhaler. The type of isotope depends on which organ is being examined. For whole body PET CT, 18F-fluorodeoxyglucose is most commonly used.
Penetrating into the body, the radiomarker emits energy of different frequencies. Metabolic rates differ between altered and healthy tissues. In places where tumors are localized, active uptake of glucose and increased cell division are observed. It is these processes that are recorded by sensors. When deciphering the results, doctors analyze the sections obtained and determine the degree of accumulation of radioactive particles in the tissues. A PET scanner determines the foci where the largest amount of isotope accumulates, and a computed tomograph determines their location.
Advantages of PET diagnostics:
- high reliability of diagnostic results;
- the ability to detect tumors at an asymptomatic stage;
- no age restrictions;
- painlessness and safety;
- possibility of simultaneous examination of different organs.
Areas of application of PET CT in medicine
About 80% of all clinical PET CT studies are performed in oncology. Today, this is one of the most accurate and informative ways to diagnose cancer. Positron emission tomography makes it possible to differentiate tumors, determine the extent of their spread, and identify metastases at an early stage.
In cardiology, the study makes it possible to assess the condition of the heart muscle, detect areas with impaired blood circulation, and identify signs of heart attacks and coronary artery disease that were not diagnosed in time at an early stage.
The effectiveness of PET examination in neurology has been proven. Without surgical intervention, doctors are able to record changes characteristic of epilepsy, Parkinson's and Alzheimer's diseases, multiple sclerosis and other complex disorders.
Differences between PET CT and other diagnostic methods
Positron emission tomography has a number of advantages over traditional scanning methods (X-ray, ultrasound, MRI, etc.). The main advantage of PET CT is the ability to accurately determine oncological processes.
The hybrid PET CT method detects tumors and metastases more accurately than other research methods, determines the location of pathological foci and the extent of pathological changes.
When examining different parts of the body using X-rays, it is often necessary to perform several scanning procedures, which increases the radiation dose to the body and increases the cost of diagnosis. Using a PET scanner, during one procedure, you can examine all organs and parts of the body at once.
The study lasts 40–60 minutes, decoding the images takes from 3 hours to 2 days. The results are given to patients on a CD or in printed form. The examination report is accompanied by a doctor's report.
Indications for the study
- Search for the primary tumor site when metastases are detected;
- Determination of the stage of the oncological process;
- Differentiated diagnosis of relapse and post-treatment changes;
- Monitoring the course of the disease, detecting relapse;
- Planning of radiotherapy and surgical manipulation;
- Planning a biopsy and finding the most aggressive area of the tumor.
Radiofrequency ablation of liver metastases
Preparation
When preparing for the examination, you must adhere to a number of rules:
- The day before your scheduled procedure, follow a low-carbohydrate diet.
- Come to the examination on an empty stomach.
- On the eve of the study, avoid heavy physical activity.
- On the day of the procedure, drink plain water.
- Stop chewing gum.
- Come to the procedure in comfortable, comfortable and preferably warm clothing.
It is recommended to bring information about the disease, diagnoses, extracts from other hospitals, results of other studies, etc. to the research procedure.
Carrying out
The procedure itself takes about an hour, but it is necessary to keep in mind the preparation, preparation of the necessary papers and post-procedure rest.
The procedure is carried out in comfortable clothing; it is necessary to remove everything containing metal.
It is necessary to inform your doctor about the pain that may arise from prolonged immobility. Taking this into account, he will be able to select an individual procedure for the procedure.
After the injection, you must lie silent, motionless and relaxed. Immobility has a beneficial effect on the correct distribution of the administered drug. This is important for image quality.
The first stage of the examination is the administration of the drug. It lasts about an hour. The drug is administered intravenously. Sometimes the patient may feel fever, nothing more. The distribution of the drug among the cells lasts about an hour.
The second stage is scanning. Patient in a tomograph. CT is performed first, then PET. If required, an additional contrast agent is administered. The duration of this stage varies from twenty to forty minutes.
Upon completion, the CT and PET images are superimposed.
Positron Emission Tomography (PET)
- Seal
Positron Emission Tomography (PET)
It is an additional diagnostic method for assessing metabolic disorders and localizing epileptogenic zones.
In clinical practice, PET is most often used using fluorin-8-fluoro-2-deoxy-D-glucose (18-fluorodeoxyglucose). The epileptogenic zone is characterized by hypometabolism in the interictal period and hypermetabolism during an attack.
This method is most sensitive when epileptogenic changes are located in the temporal lobes of the brain.
PET, in particular PET-CT, provides better image quality and higher resolution compared to SPECT. To study epilepsy, various types of PET are used: based on the metabolism of glucose, serotonin, oxygen, blood flow speed and receptor density. Fluoro-2-deoxyglucose (F-FDG) PET, based on the assessment of glucose metabolism in the brain, is a proven and relatively affordable method. Other PET studies place great demands on equipment, technical personnel, and, accordingly, are expensive.
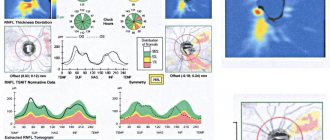
Figure 1. FDG-PET shows a large area of hypometabolism in the right temporal lobe (arrows) (A). FMZ-PET shows a more precisely localized area in the mesial temporal region in the same patient (arrow) (B). Symmetrical distribution of FMS in a healthy person
FDG-PET is a method based on studying the metabolism of a radiosensitive analogue of glucose. Glucose is the main source of energy for the brain. Glucose metabolism is directly dependent on neuronal activity. F-FDG enters cells from the blood using transmembrane transporter proteins, in particular GLUT1. In the cell, F-FDG is phosphorylated by hexokinase to FDG-6-phosphate. Further metabolism of FDG-6-phosphate is limited and, in essence, the molecule remains locked in the cell.
The study is carried out on an empty stomach; the day before the test you should not drink alcohol, coffee, or drugs that affect brain activity. 30 minutes before and 30 minutes after the FDG injection, the patient should be in a quiet environment, excluding noise, bright light and other irritants. If the blood glucose level before injection exceeds 150-200 mg/dL, the test is postponed, because in a state of hyperglycemia, high levels of circulating insulin increase the transport of FDG into the muscles and reduce its uptake by the brain. In patients with diabetes mellitus, the success of the study depends on the degree of diabetes compensation. Before FDG administration, a low-dose CT scan is performed with subsequent processing. The FDG dose for adults is 185-740 mBq, for children 5.18-7.4 mBq. The dose is reduced when using 3D scanning, which is possible with most modern devices. FDG-PET is performed 30-60 minutes after FDG injection and lasts 15-30 minutes. When performing PET-CT with a high dose of FDG - 740 mBq, the examination time is reduced to 5 minutes.
Figure 2. FDG-PET in a 1-year-old child with tuberous sclerosis. (a) FDG-PET shows multiple foci of decreased metabolism, with the greatest decrease in the right parasagittal region of the frontal lobe (arrows). (b) CT scan shows sclerosis in the right parasagittal region of the frontal lobe. (c) FDG-PET/CT shows that the area of maximum metabolic decline corresponds to the right parasagittal region of the frontal lobe.
Normally, in the adult brain, there is high FDG uptake in the cerebral and cerebellar cortex, as well as moderate uptake in the white matter. FDG uptake in children varies depending on age. Infants tend to show widespread low metabolic activity. After reaching 4 months of age, there is a sharp increase in glucose metabolism and reaches its peak around 4 years of age, decreasing slightly thereafter as age increases. As we age, metabolism normally decreases in the lateral and medial frontal cortex, as well as in the anterior lumbar cortex. Pathologically altered regions are characterized by an increase, decrease, or absence of metabolic activity. Semi-quantitative tests help detect local or global abnormalities that are not noticeable on conventional neuroimaging. Semi-quantitative analyzes involve comparison of FDG uptake in a region of interest with the overall metabolic pattern. They can be done manually or using special programs. Integration of FDG-PET and MRI is possible, which increases structural and functional information content. Quantitative analysis (absolute glucose metabolism) requires blood sampling (arterial) with dynamic measurement. Thus, in clinical practice, most centers favor simplified protocols and static images. PET images are usually obtained in the interictal phase, characterized by focal hypometabolism. Carrying out PET scans during the ictal period is difficult because seizures are difficult to predict and they take a short time (with the exception of epi-status). Another limitation of ictal PET is the prolonged (30–45 min) brain uptake of FDG after injection, which is caused by complex patterns of increases and decreases in metabolism. Postictal PET demonstrates complex patterns of metabolic changes or focal changes.
A large number of clinical studies demonstrate that FDG-PET is highly sensitive for localizing drug-resistant epilepsy, even in the presence of equivocal MRI and EEG findings.
The sensitivity of FDG-PET is maximum for temporal lobe epilepsy (87-90%) and decreases for extratemporal epilepsy (38-55%). PET allows making the final decision when selecting candidates for surgical treatment in 53% of cases with normal or inconsistent MRI. In children, MRI is ineffective in diagnosing discrete lesions in extratemporal epilepsy. At the same time, the sensitivity of FDG-PET is 92%, and the specificity is 62.5%
Large studies suggest that FDG-PET should also be preferred over SPECT in the interictal period. Interictal PET is very sensitive in the lateralization and localization of the epileptogenic focus, but this study is not enough to determine the extent of resection, since the zone of FDG hypometabolism extends beyond the boundaries of the altered tissue. For this reason, FDG-PET does not always differentiate mesial temporal lobe epilepsy from lateral temporal lobe epilepsy.
Figure 3. PET scan for epilepsy. Epileptogenic focus in the form of a hypometabolic zone in the right temporal lobe (arrows).
There are few observations of PET during the ictal period. Most ictal PET scans were performed in patients with status epilepticus and those with artificially induced seizures. For example, in a patient with amusia, PET performed during the ictal period showed hypometabolism in the lateral parts of the right temporal lobe, with a simultaneous increase in metabolism in the anteromesial parts of this lobe of the brain.
Postictal PET scans showed that metabolic rate varied with the timing of FDG injection after the attack. In the early postictal phase (FDG injection within 15 minutes of the attack), PET shows focal hypometabolism. The peak decrease in metabolism is observed 48 hours after the attack. The metabolic rate was intermediate in the first 24 hours. Some authors believe that after a partial attack, the level of glucose metabolism in the affected cells may return to baseline levels within 24 hours.
In addition to localizing the epileptogenic focus, preoperative PET provides important information about the functional state of the brain as a whole. Interictal FDG-PET is the best method for visualizing the area of functional deficit (ZFD). The DFD is presented as a brain region with altered metabolism in the interictal period. Extratemporal hypometabolism is a poor predictor of outcome after surgery. Localization of the epileptogenic focus can be complicated by the presence of a bitemporal zone of hypometabolism in unilateral lesions. In this case, a PET scan is recommended 2 days after the attack. Areas of hypometabolism in the frontal lobes in temporal lobe epilepsy are a result of the depression that often develops in these patients.
Receptor PET
Figure 4. C-WAY-100635 PET scan in a patient with MRI-negative temporal lobe epilepsy. And the EEG is focused in the right temporal lobe. A. T1 axial MRI shows no structural abnormalities. B. C-WAY-100635 PET shows asymmetrical loss of density in both the lateral and mesial temporal lobes.
In epilepsy, changes also occur at the level of receptors and neurotransmitters. According to modern concepts, changes in neuronal activity are caused by a violation of the ratio of excitatory and inhibitory neurotransmitters. Excitatory glutamatergic neurotransmission, particularly excessive activation of glutamate receptor 5 (mGluR5), is responsible for seizure initiation and propagation. One of the most studied neurotransmitters that plays a role in the etiology of epilepsy is γ-aminobutyric acid (GABA). GABA synaptic inhibition is known to be critical in the etiology of epilepsy. Endogenous opioid peptides are also involved in epilepsy, acting as an anticonvulsant and limiting electrical activity. An increase in serotonin levels may occur in epilepsy. In experimental models, serotonin exerts anticonvulsant effects through 5-HT1A receptors. Alterations in different dopamine receptor subtypes, especially D1 and D2, are associated with various forms of epilepsy.
Figure 5. Interictal O-H2O PET in a patient with bitemporal temporal lobe epilepsy. There is hypoperfusion of the temporal lobes compared to the rest of the brain.
Numerous adenosine receptor subtypes have been implicated in epilepsy. In particular, the A1 subtype plays a role in the regulation of seizure activity. Histamine 3 receptor subtype, nicotine-sensitive and muscarine-sensitive acetylcholine receptors are also implicated in the pathophysiology of epilepsy.
Figure 6. Increased cortical AMT uptake (arrows). A. Hyperintense area in the right perisylvian cortex. B. Hyperintense signal in the left temporal lobe cortex in another patient.
Receptor PET has been used to assess the role of neurotransmitters in the epigenesis and propagation of epileptic activity, as well as to localize epileptogenic regions and plan new treatment approaches.
What after?
Afterwards, it is not recommended to be in crowded places for 24 hours, especially to have contact with pregnant women and children. In the family, it is necessary to maintain a social distance of 1 -1.5 from each other.
It is necessary to consume a lot of fluid, two and a half liters or more. This is necessary to remove contrast and radiopharmaceuticals faster and safer.
You can drink any decaffeinated drinks, not just water.
Complications
Complications during the examination procedure are mainly associated with the administration of contrast.
It could be:
- Allergy caused by vein puncturing;
- Damage to blood vessels;
- The appearance of a hematoma;
- Neuritis
A very rare complication is renal dysfunction.
Oral administration of contrast may cause nausea, vomiting, and diarrhea.
After the procedure, dizziness and weakness may occur due to the fact that the stomach is empty.
Radiation exposure to the patient during examination
The choice of radiation dose is influenced by the radiopharmaceutical used and the scope of the study. So scanning the head requires less radiation than scanning the whole body. Minimizing harm from using the method is achieved if the following requirements are followed:
- Use isotopes with a half-life of several minutes or hours;
- Calculate the dose individually for each patient, taking into account his age, height, weight;
- Use special filters on scanners, as well as programs that reduce radiation doses;
- Consume the required amount of fluid, this will allow you to quickly remove the radiopharmaceutical from the body
By contacting the Onco.Rehab integrative oncology clinic, you will find out where it is best to undergo the study that we told you about in this article.
Neuroscience for everyone. Methods: positron emission tomography
Medicine knows many cases where apparently healthy people were found to have advanced malignant tumors either affecting many regional lymph nodes or even with metastases to other organ systems. At the same time, people previously could even be examined by taking an X-ray or performing a CT scan. Brain tumors - for example, gliomas - are seen very accurately by MRI. But sometimes, in order to find a tumor process at an early stage of development, even ultra-precise “photographs” of internal organs are not enough. In addition, I really want to see the activity of the brain - and functional magnetic resonance imaging may not be enough. And then positron emission tomography or simply PET comes into play (not to be confused with the bottle material - polyethylene terephthalate!).
Positron emission tomogram
Surprisingly, the first works on PET appeared almost earlier than attempts to create magnetic resonance or even computed tomography. The same can be said for working prototypes. The seminal article on PET appeared in 1975 in the journal Radiology. It's hard to believe, but more than 40 years ago the first prototype of a tomograph was built. True, then it was called PETT - positron emission transaxial tomograph. See what this prototype looked like, created by Michael Ter-Poghossian and his colleagues. Using his example it is good to show the principle of operation of PET.
First PET prototype
It seems incredible, but the main physical principle in PET is the annihilation of matter and antimatter. We need a short-lived isotope that decays by beta(+) decay, emitting a positron, the antiparticle to the electron, discovered in 1932 in cosmic rays. We make an organic molecule labeled with an atom of this isotope - a so-called radiopharmaceutical (RP), which is introduced into the body. In the body, an atom disintegrates; a positron, colliding with the first atom on its way, interacts with an electron. They annihilate, emitting two energetic photons - gamma rays.
So, here, in the prototype, the sample is simply tissue with a radiopharmaceutical or an animal into whose blood the drug has been injected, surrounded by 24 hexagonally arranged scintillation detectors (six groups of four detectors) based on thallium-activated sodium iodide. When a gamma ray hit them, a glow appeared in the crystals, which was detected by a photomultiplier. Based on which detectors “turned on,” it was possible to determine from which point of the analyzed sample or animal two gamma quanta emitted, simply by drawing straight extensions of the detector tubes until they intersected. Surprisingly, even with such primitive devices it was possible to obtain images. Here, for example, is an image of a dog's vertebra.
Now the principle is the same, only there are more detectors and they are located in the “pipe” of the tomograph. The detectors themselves are scintillation counters - gamma rays passing through crystals, for example, lutetium oxyorthosilicate Lu2SiO5, cause a glow that is recorded by photomultipliers.
PET operation scheme
So, positrons are delivered to the body using special radiopharmaceuticals (RP), which are any biologically active substance labeled with a positron-emitting isotope during beta (+) decay. The substance is selected depending on what process is being studied: gene expression, intracellular metabolism, or the transport of various substances throughout the body. This diversity makes PET a fairly universal diagnostic tool, which helps make an accurate diagnosis not only in oncology, but also in cardiology, neurology or endocrinology.
In neuroimaging, the most commonly chosen biologically active compound is glucose, which is labeled with the fluorine-18 isotope with a half-life of just over 109 minutes. Our brain takes up only two percent of our body weight, but consumes 20% of our total energy. And it takes energy from glucose. Therefore, to study the brain, fluorine-18 is first produced in a cyclotron, then fluorodeoxyglucose (FDG) is synthesized, in which one –OH group is replaced by 18F. PET is also used to diagnose Parkinson's disease, and then a radiopharmaceutical based on levodopa is synthesized.
Fluorodeoxyglucose
After this, the radiopharmaceutical must be delivered as quickly as possible to the diagnostic center, where it will be administered to the patient and the registration procedure will be carried out. Large PET centers have their own cyclotrons, which makes the situation easier, but there are countries in which radiopharmaceuticals are made centrally and then transported by plane to medical centers.
The procedure takes about one and a half to two hours. A little more than half an hour is allotted for the distribution of the drug throughout the tissues, and then the person is placed on the scanning machine couch and the picture of the metabolic activity of the tissues is visualized. The affected organs absorb the drug most strongly, a greater amount of energy is released in their area, so they begin to glow in the image, thus marking the problem. In order to achieve special accuracy, during PET a computed tomography is performed, and the images are superimposed on a color image of the metabolism, allowing you to see the location of the lesion as clearly as possible and already formulate treatment tactics.
Whole body PET scan with FDG
If we examine brain activity, PET provides better resolution and shorter time delay than fMRI. There is only one thing that prevents the widespread use of this method in neuroscience: it is very expensive.
PET has several main advantages: firstly, the method allows you to examine all organs at once, while having a radiation dose comparable to CT. Secondly, he “sees” the slightest shifts in tissue metabolism long before an organic focus is formed. This is beyond the power of conventional X-rays, ultrasound, or even MRI. Thirdly, positron emission tomography can determine the size of even minor metastases up to several millimeters in diameter, clarify their location, and also monitor the effectiveness of the prescribed treatment. By the way, the accuracy of standard CT fluctuates within 80%, while the accuracy of PET reaches 90-95% with the same safety and painlessness.
But there are also disadvantages. Firstly, the need for rapid delivery of the radiopharmaceutical. Of course, the half-life of 18F does not mean that after 109 minutes you will have nothing left, but, nevertheless, the drug's activity is halved during this time. Well, besides, the method is very expensive, because radiopharmaceuticals are prepared for each specific patient literally before the procedure. PET-CT of the brain in Russia costs more than 40,000 rubles. You shouldn’t think that it is cheaper in other countries, on the contrary: the recommended price in the UK is about 700 pounds sterling, in Canada – 1200 Canadian dollars.
In addition to neuroscience and oncology, positron emission tomography can detect disturbances in the blood supply, so it can be used to diagnose cardiac ischemia, and also with its help to find old myocardial infarctions by areas of reduced blood flow. PET is also productive in clinical neurology: it perfectly identifies foci of increased activity in epilepsy, which makes it possible to clarify the scope of surgical intervention, as well as to find at an early stage and make a differential diagnosis between different neurodegenerative diseases.
PET-CT images
PET-CT scanner
It must be said that PET has received further development in the 21st century. In 2000, an article was published that described the combination of PET and computed tomography (PET-CT), and in 2008, the combination of PET with MRI. Now PET/CT has already become the gold standard in some types of studies, and serial PET/MRI units have also appeared.
Text: Anna Horuzhaya, Alexey Paevsky